Health
Mak Researcher Designs “COVID Alphabet” for Awareness and Behavioral Change

By Joseph Odoi
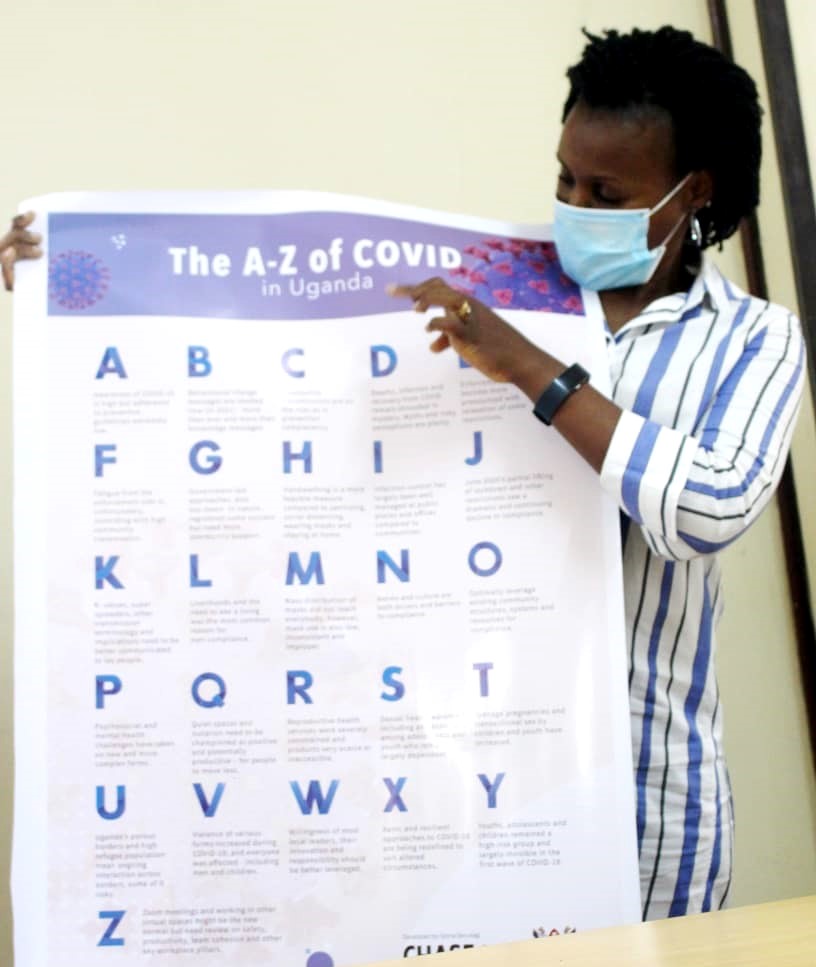
With the increasingly worrying situation of the novel coronavirus and its devastating global effect, Makerere University has once again taken an institutional lead by designing a behavioral change communication model to support government efforts in fighting against the pandemic. The COVID Alphabet (A-Z of COVID in Uganda) was developed by Dr. Gloria Seruwagi, a lecturer at Makerere University’s College of Humanities and Social Sciences (CHUSS) and School of Public Health (MakSPH).
While briefing journalists during the model’s unveiling at Makerere University on February 17th, 2021, Dr. Seruwagi shared that she got the inspiration to design the simple and relatable evidence-based product after conducting a series of COVID-19 studies in different communities including the REFLECT study in humanitarian contexts and ALERTs study in different informal settlements within Kampala.
“If somebody wants to know what the key issues are about COVID-19 in Uganda, they can look at this Alphabet and have it all at a glance, without having to go through the long process of reading a 4 or 15-page document. This is not just an alphabet for learning phonetics or numbers. It is a Know, Think and Act (KTA) tool packed with nuggets of information” Dr. Seruwagi emphasized.
The COVID Alphabet is not only easy on the eye and deliberately simple but is also factual and anchored in research. It should resonate with anyone at any level – from the busy policymaker or program manager to someone outside Uganda in need of quick facts.
The Alphabet also speaks to today’s virtual workplace teams, community leaders, and any person on the street or at home. It contains critical study findings compressed into a quick and concise summary of the COVID trajectory, experiences, and outcomes. It also gives key pointers on key population groups, sectors, mitigation strategies, and action points for different stakeholders.
The Alphabet begins by stating that Awareness of COVID-19 is high but Adherence extremely low. It then flags up the increasingly urgent need for effective Behavioral change messages now more than ever, even more than knowledge-only messages. Community transmissions are on the rise; as is prevention complacency while Deaths, infection and recovery from COVID-19 remain shrouded in mystery.
Uganda continues to face another battle of the serious infodemic challenge with myths, falsehoods and risky perceptions being plenty. Enforcement fatigue has become more pronounced with relaxation of some restrictions and unfortunately Fatigue from the enforcement side is coinciding with high community transmission. The Alphabet acknowledges the important role and success registered by Government-led approaches; however, it shows that these more community support and leadership.
Hand washing is listed as a more feasible prevention measure compared to sanitizing, social distancing, wearing masks and staying at home. This is in harmony with research carried out by other studies which showed that hand washing was the most adhered to guideline at the peak of COVID-19 as most households had hand washing points.
Dr. Seruwagi says adds that Infection control has largely been well managed at public places and offices compared to communities. And while the model recognizes that mass distribution of Masks did not reach everybody; mask use among those who have is low, inconsistent and improper.
This also alludes to study findings which found a lot of negative face mask practices including chin-masking, sharing masks, wearing ill-fitting masks, keeping them in pockets and back or not having a mask at all. Moving forward, Seruwagi advises the government to not only give out masks but revitalize enforcement of SOPs, reminding people of the dangers and health risks posed by the pandemic.
Norms and culture are both drivers and barriers to compliance. This alphabet statement agrees with research findings which show that the practice of hand washing with soap was much higher in Muslim communities because it’s in tandem with their beliefs and socio-cultural practices. The model also highlights the need to Optimally leverage existing community structures, systems and resources for compliance.
Since the outbreak of COVID-19, Psychosocial and mental health challenges that have taken on new and more complex forms. And while the need for social networks and connections is very important, Dr Seruwagi also recommends that Quiet spaces and isolation should be championed as positive and potentially productive.
This is in line with trying to get the community avoid unnecessary movement and avoid or behave responsibly while in public gatherings. It will enable communities to not feel punitively restricted but rather appreciate the protective effect of measures such as curfews.
In terms of Reproductive health, the Alphabet shows that services are severely constrained and products very scarce, inaccessible or expensive. Related to this is that the pandemic has worsened SRH outcomes, especially among adolescents and youth since the advent of the pandemic.
Teenage pregnancies and transactional sex by children and youth have increased; calling for parents, teachers, leaders and other stakeholders to act. ‘’If we are saying that there is a lot of teenage pregnancies and transactional sex by adolescents, what should teachers do, what are parents doing to protect their children?” she remarked in a call for action.
Dr. Seruwagi’s landmark model then turns to the country’s globally lauded success in refugee-hosting. It highlights the Uganda’s porous borders and high refugee population, noting that this comes with daily interaction across borders and some of this interaction risky with potential for disease transmission and other risks beyond health for example security risks.
The model shows that Violence of various forms increased during COVID-19; and everyone was affected including men and children. In some of the studies conducted, Violence against Men (VAM) is emerging as a key theme but the Ugandan culture largely operates in a culture of silence and there are not enough or effective services addressing male survivors of violence – most interventions have focused more on women. Moreover, child protection systems were rendered more fragile by the pandemic.
All these services and intervention points need strengthening. The Willingness and resourcefulness of community leaders needs to be harnessed and effectively utilized. And Dr Seruwagi says that the timing is a good one in terms of policy implementation, with the recent launch of the Community Engagement Strategy where VHTs, community leaders and other local structures are critically positioned to make a significant contribution if well-resourced and supported. It mentions Xanic and resilient approaches for COVID-19 while also highlight children, adolescents and Youth as a severely-affected but largely “invisible” group during Uganda’s the first wave.
Finally, the model recognizes the role of technology like Zoom meetings and while it acknowledges that virtual spaces are the ‘new normal’, Dr Seruwagi calls for a thorough and ongoing review on their safety and impact on productivity or team cohesion. “For example, the people delivering essential services needed during these difficult COVID times might, themselves, be in serious need of mental health and psychosocial support or specific workplace provisions,” she said.
Dr. Seruwagi implored leaders, teachers, parents, civil society organizations, policymakers and all health stakeholders to pick an action point from each Alphabet letter to implement if COVID-19 is to be countered. “As a country we already crossed a line where infections were managed at facility level. With the current community spread, let’s reflect on this COVID Alphabet and let each person pick at least one action point”. She called upon senior policymakers and BCC specialists to take up the model as guiding tool to support the national response.
The COVID Alphabet is the first of its kind in Africa and has attracted media attention with different people describing it as factual, precise, simple and easy to understand.
Article originally published on MakSPH











Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General7 hours ago
General7 hours agoUndergraduate Admission Lists 2026/2027
-
 General6 days ago
General6 days agoFreshers’ Joining Instructions 2026/2027
-
 General1 week ago
General1 week agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General1 week ago
General1 week agoMakerere University Welcomes 2026/2027 Freshers
-

 General7 days ago
General7 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training