Health
New Uganda study shows Oxygen Access increase among neonates & children in Hospitals

A new study in Uganda has shown a significant increase in oxygen access and pulse oximetry among neonates and children in health facilities.
Preliminary findings published in The Lancet, the world’s highest-impact medical and academic journal show the positive impact of a diverse oxygen systems strengthening intervention on diagnosis, oxygen therapy use, and mortality rates.
Titled; “Improving Effective Coverage of Medical Oxygen Services for Neonates and Children in Health Facilities in Uganda: A Before-After Interventional Study,” the study shows that large-scale improvements in hospital oxygen services are achievable in a relatively short timeframe and have great potential for impact.
The study was led by Dr. Freddie Ssengooba, an Associate Professor of Health Policy Planning and Management, at the School of Public Health and Dr. Freddy Eric Kitutu, a Senior Lecturer of Health Systems Pharmacy both co-chairs of the Lancet Global Health Commission on Medical Security. Other researchers on the study include Hamish Graham from the University of Melbourne, Yewande Kamuntu, Blasio Kunihira, Santa Engol, Jasmine Miller, Absolom Zisanhi, Dorcas Kemigisha, Lorraine Kabunga and Felix Lam all from Clinton Health Access Initiative, Dr. Charles Olaro from Uganda’s Ministry of Health and Dr. Harriet Ajilong from the Uganda Paediatric Association.
From June 2020 to June 2022, an intervention study assessed neonates and children at 31 government health facilities in Uganda’s Busoga and North Buganda regions, located at altitudes of 1100-1400 meters. The primary outcome measured the proportion of patients with documented pulse oximetry on admission.
Secondary outcomes included patients with severe hypoxaemia (SpO2 < 90%) receiving oxygen, overall oxygen usage, and appropriate oxygen usage. The study’s primary effectiveness analysis compared pulse oximetry coverage before and after the intervention, incorporating a 4-month washout period. The analysis utilized mixed-effects logistic regression, adjusting for clustering at individual facilities, age (child versus neonate), and sex (male versus female).
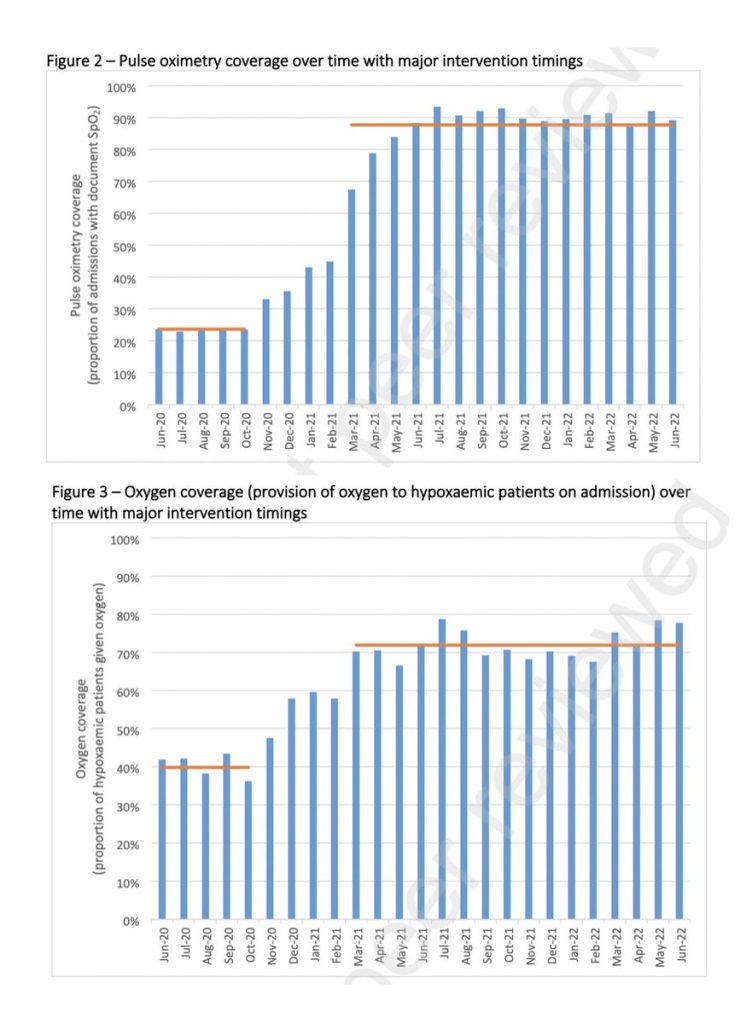
Researchers analyzed 64,562 patients (25% neonates) and observed a significant rise in pulse oximetry coverage during the intervention period, increasing from 24% to 88% with an adjusted odds ratio of 40.1 (95% confidence interval: 37.4 to 42.9).
They also observed better oxygen coverage for children and neonates with low oxygen levels, increasing from 40% to 71%, with an adjusted odds ratio of 3.81 (95% confidence interval: 3.26 to 4.46).
Additionally, there was a slight increase in overall oxygen usage, rising from 8% to 11%, with an adjusted odds ratio of 1.95 (95% confidence interval: 1.79 to 2.13).
“Improvements were relatively greater in smaller facilities and for children (versus neonates). We estimated additional patients served and lives saved in the post-intervention period using observed effect estimates in this and other studies,” reads the study.
With these findings, researchers are calling on governments in low-income and middle-income countries to create oxygen plans and invest in proven solutions, like incorporating pulse oximetry in regular hospital care, and providing clinical as well as biomedical mentorship and support.
For all age groups, medical oxygen is essential for both acute and chronic health problems. Scientific evidence suggests access to medical oxygen services that are safe, economical, and appropriate is essential for improving overall health and achieving Sustainable Development Goals. Unfortunately, inadequate or inconsistent oxygen supplies present challenges for many low- and middle-income nations, particularly for small medical facilities in underserved areas.

Disruptions in the oxygen supply during the COVID-19 pandemic caused excessive deaths, which predominantly affected countries with low to middle incomes. According to a 2021 study, half of the COVID-19 patients who died in 64 critical care units across ten African countries did not receive the required medical oxygen.
The study was funded by a grant from the Bill and Melinda Gates Foundation (BMGF) and ELMA Philanthropies to the Clinton Health Access Initiative (CHAI) and approval from Makerere University School of Health Sciences Research and Ethics Committee, and the Uganda National Council of Science and Technology.
Available at SSRN: https://ssrn.com/abstract=4676954 or http://dx.doi.org/10.2139/ssrn.4676954










Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.


-

 General3 days ago
General3 days agoUndergraduate Admission Lists 2026/2027
-
 General1 day ago
General1 day agoFreshers’ Joining Instructions 2026/2027
-
 General2 days ago
General2 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General3 days ago
General3 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General1 week ago
General1 week agoCall for Erasmus+ Mobility Exchanges between Makerere University and University of Perugia