Health
MakSPH Champions Leadership Boost for Wakiso Health Managers
On April 23, 2025, Makerere University School of Public Health (MakSPH) convened district leaders, health managers, and project partners to disseminate the outcomes of a major leadership and management strengthening initiative in Wakiso District, Central Uganda. The one-year project, part of the Global Health Partnerships programme funded by NHS England, was implemented in collaboration with Nottingham Trent University, Nottingham University Hospitals NHS Trust, Wakiso District Local Government, and Uganda’s Ministry of Health.
Launched in 2024, the project titled Strengthening Leadership and Management Among Local Government Health Managers in Wakiso District, aimed to co-design and pilot a leadership and management training tailored to the realities of Uganda’s decentralised health system. The intervention, led by Makerere University’s Dr. David Musoke and Nottingham Trent University’s Prof. Linda Gibson, through the over 15-year-old NTU-Mak Partnership impacting lives in Wakiso, began with a field visit to over 60 public health facilities in the district, a needs assessment within these facilities to identify key priority gaps, and a baseline survey with the health in-charges to establish the initial status of key indicators.
“We have been very fortunate to work with a supportive local government in Wakiso, from the top leadership down. While many projects struggle to engage district teams, our longstanding relationship with Wakiso made collaboration seamless. Although this was our first initiative specifically focused on leadership and management, we hope it will serve as a stepping stone for even more impactful work in the future,” Dr. David Musoke, a Senior Lecturer at Makerere University and the Uganda Project Lead, said during the dissemination workshop, highlighting the key success factors for the leadership and management project.

Initial results from the needs assessment and baseline on leadership and management competencies conducted among Wakiso District health facility supervisors early last year by the project team and shared during the three-day workshop in June 2024, held in Kampala, which kickstarted the six-month structured fellowship programme for 53 health managers in Wakiso, had found critical capacity gaps. Using a tool evaluating 17 leadership and 33 management competencies, only 40% of the managers met the 80% benchmark for leadership, scoring highest in cognitive skills, while just 33% met the required management standard, performing best in self-management and lowest in quality management.
Then, the health facility managers with postgraduate training, longer service, and strong team dynamics, showed overall better performance. While working relationships with subordinates and the district leadership were largely positive, performance was hampered by systemic challenges such as limited resources, low motivation, and weak teamwork. Overall, the study also pointed to a misalignment of expectations between the District Local Government and the Health Ministry, underscoring the need to strengthen coordination to improve services.
The result of this mismatch was to the effect that, as of this time last year, Wakiso District ranked among the bottom 10 on the national health league table, which is an annual Ministry of Health assessment of district performance across key service delivery and patient satisfaction indicators. This was despite Wakiso being Uganda’s most populous district, with over 3.4 million residents today, as it continued to struggle to deliver essential health services to the public. The 2022/2023 Annual Health Sector Performance Report also flagged persistent challenges, including frequent transfers of facility in-charges, overstretched management structures, and weak internal communication and coordination.

It was this stark reality that informed the leadership and management intervention in Wakiso. Officiating the dissemination of the project outcomes, Dr. Sarah Byakika, Commissioner for Planning, Financing, and Policy at the Ministry of Health and a member of the National Oversight Mechanism for the programme, commended the remarkable progress made in just six months, citing visible improvements across the district as a direct result of the intervention.
“I have been involved with this programme right from its inception, and I’m proud that Uganda became one of its major beneficiaries,” Dr. Byakika said with gratitude, commending the strong collaboration between the Ministry of Health, Makerere University, Nottingham Trent University, Nottingham University Hospitals, Wakiso District and the development partners for supporting the initiative. She emphasised the value of this partnership in strengthening leadership and management competencies among Wakiso District health managers to address critical performance gaps in health service delivery.

“Wakiso is Uganda’s largest and most populous district, yet it has long underperformed on key health indices. Despite its semi-urban nature, it faces enormous health service delivery challenges, partly due to the overwhelming burden on its District Health Officer, who oversees more than 60 public and over 340 private health facilities. Many of these private facilities open and close frequently, complicating service oversight,” Dr. Byakika observed with concern.
Her sentiments were echoed by the District Health Officer, Dr. Emmanuel Mukisa, in a message delivered by Wakiso District Biostatistician, Mr. Frank Kakande. He noted that the project had contributed to a noticeable shift in the district’s health system performance, with visible improvements in leadership, communication, and accountability among facility in-charges beginning to translate into better overall health service delivery outcomes.
“You cannot talk about management without addressing performance: they go hand in hand. As someone who sits at the centre of district health data, I can confidently say that performance has improved. During the most recent national local government performance assessment, where I participated in the evaluation, Wakiso District’s health department ranked 18th out of 146 districts. That health ranking is a major achievement. We have consistently performed poorly in the past, but this time, we made significant progress,” Mr. Kakande told the attentive audience, speaking with an air of relief and satisfaction.

The Wakiso District Biostatistician credited part of this progress within the district, from the poor performance last year, to the leadership training and mentorship delivered through the project, citing visible improvements across key health indicators. He stressed the need to sustain this momentum through continued mentorship, internal capacity strengthening, and consistent application of the skills acquired by health managers, particularly in tackling persistent management challenges such as absenteeism, delegation, and accountability.
“Last week, I held a performance review at Kakiri Health Centre III, and the improvements were clear. These management skills are making a difference. You can see the change across indicators. But what matters now is sustainability. The support provided through supervision and mentorship was essential. But it’s up to us to keep the fire burning. We have learned a lot: communication skills, problem-solving, time management, and decision-making. Managers are now communicating better. Even issues like absenteeism are being addressed through proper reporting and action,” Mr. Kakande said.
Earlier, Dr. Musoke, presenting the overall project overview and success, explained that based on initial findings from the baseline and needs assessment, the team co-designed and delivered a structured six-month capacity-building programme targeting 60 health facility in-charges in Wakiso District. The programme blended in-person and virtual sessions, combining practical training with one-on-one mentorship, and included an exchange component between Uganda and the UK to promote international exposure and peer learning. This allowed the health managers to apply new skills to strengthen health outcomes in Wakiso.
“This project rightly focused on addressing gaps in leadership and management. I advocated for including this component in the programme, because our national health review missions consistently show that poor performance often stems from weak leadership and management,” Dr. Byakika affirmed, adding that: “I am pleased to see that nearly all public facilities in Wakiso participated. While the project had a short implementation window, the evaluation already shows encouraging results. Health managers feel more empowered, motivated, and aware of their roles. That’s a significant step.”
For her part, Dr. Sheba Gitta, Uganda Country Director for Global Health Partnerships, formerly Tropical Health and Education Trust, applauded the leadership and management capacity-building initiative in Wakiso as a timely, locally driven intervention. She underscored the value of two-way learning between Uganda and the UK health systems through the programme, noting that Global Health Partnerships works closely with the Ministry of Health to ensure all funded initiatives align with Uganda’s national development priorities.

“What excites me most is that this was not a pre-packaged programme imported from the UK. The training was co-created by partners, based on local realities and needs. That approach reflects strong collaboration between Makerere University School of Public Health and Nottingham Trent University. I thank Prof. Linda Gibson for her continued commitment and Dr. David Musoke for his proactive leadership in bringing this programme to life. Your consistency and quality of work continue to stand out,” Dr. Gitta shared.
While commending the progress made, she cautioned against “pilotism”, as a tendency for promising projects to end prematurely, calling for the model to be scaled up nationally. To support sustainability, she stressed the importance of documenting the training process, outcomes, and costs to inform ministry-level decision-making and long-term adoption.
Dr. Gitta joined Prof. Linda Gibson, the UK Lead for the Project, to encourage the trained managers to become champions of leadership within their facilities and districts, ensuring that the impact of the programme endures beyond its current cycle. She also thanked NHS England and the UK Government for their trust and investment in Uganda’s health system.









The Democratic Republic of Congo (DRC) and Uganda recently reported an outbreak of Ebola Virus Disease (EVD), which is a serious and often deadly disease caused by a person being infected by the Ebola virus.
The virus spreads through direct contact with body fluids such as blood, saliva, faeces, vomit, urine, sweat or genital fluids from a person who is infected with EVD.
The symptoms of EVD usually develop after 8 – 10 days from contact with an infected person and may include fatigue, high fever, headache, sore throat, muscle and joint pains, vomiting and diarrhea and in severe cases, bleeding.
What should we do as the Makerere University community?
The Chief, Makerere Health Services, Prof. J.K. Byamugisha advises as follows:
- Avoid unnecessary contact such as shaking hands, hugging etc.
- Place alcohol disinfectants or hand washing equipment at all entry points within the University and ensure everyone is using them.
- Students should sit in single-person chairs while in class, avoiding contact with their neighbours.
- Do not sit too close to one another especially in frequently crowded places such as classrooms, library or any other waiting area.
- While at the University Hospital, wash hands a the gate, use alcohol disinfectant at the reception.
- All patients should have a maximum of one caretaker – others can check on them by calling.
- Avoid bringing luggage to the University Hospital.
- Target to do as instructed by the health worker.
- For further information and guidance on Ebola, please call Dr. Charles Basigara on Tel: 0702 966652 and Sr. Eunice Namubiru on Tel: 0779 950978 (Contact persons for the University Health Services)
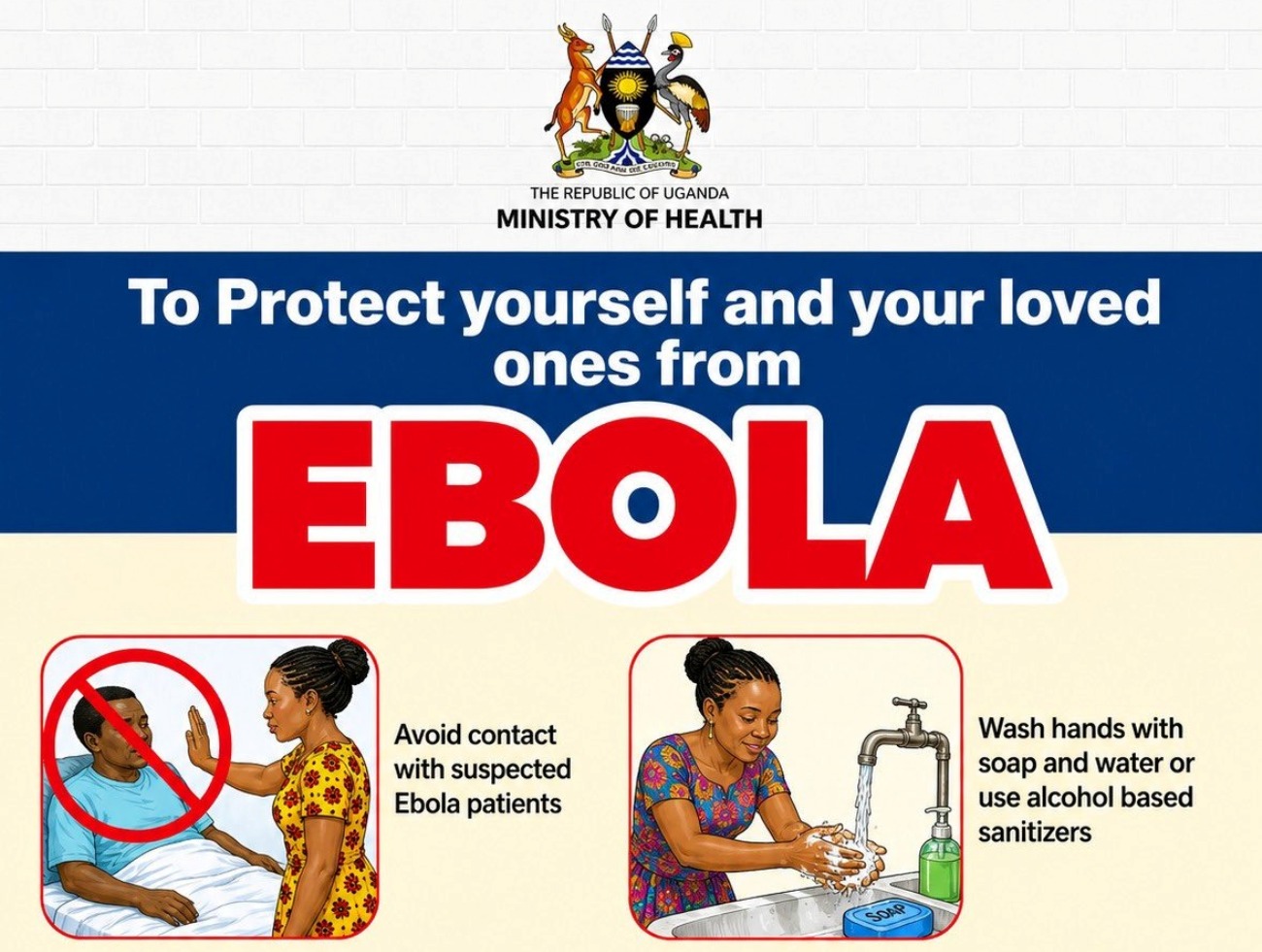
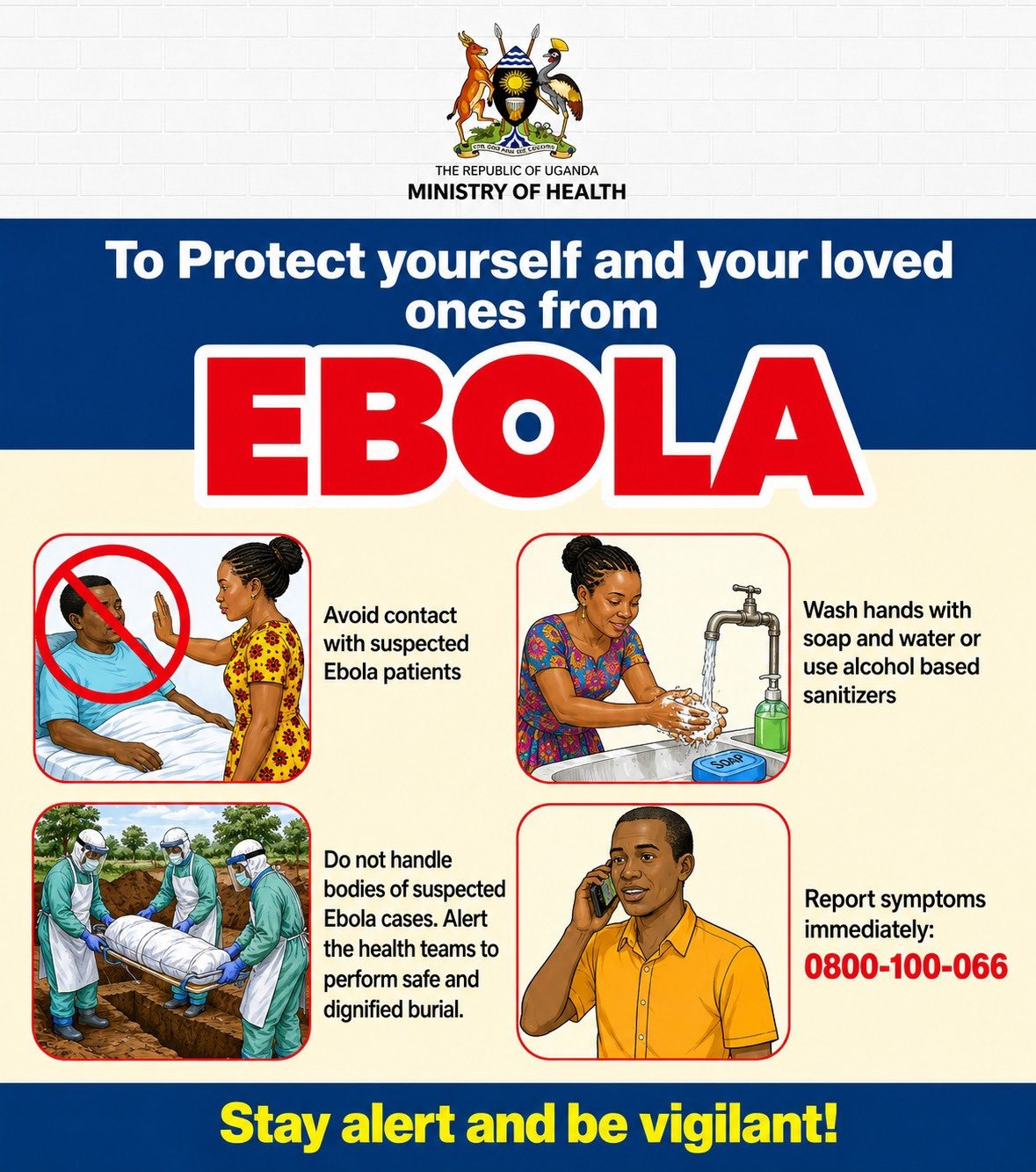
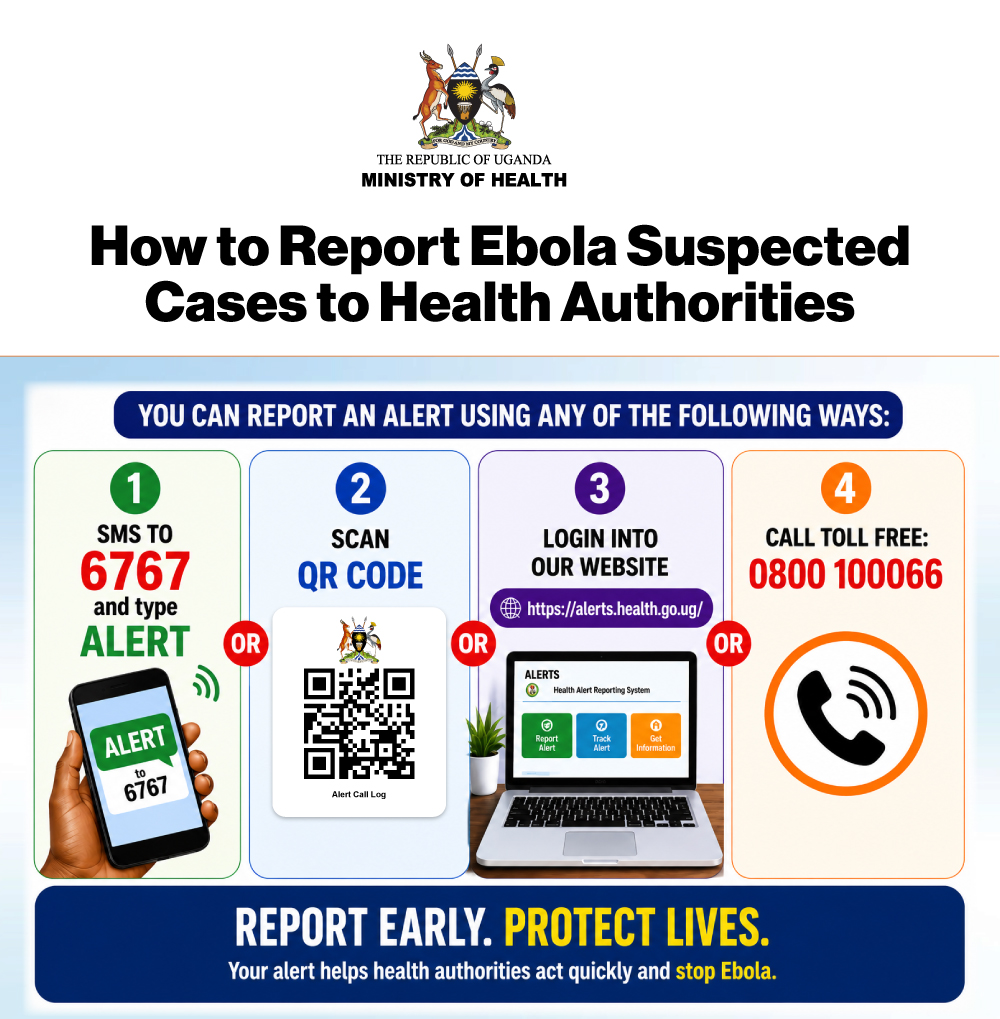
Additionally, always look out for and ensure full compliance with Ministry of Health (MoH) Infection Prevention and Control measures such as the one below.
Please find attached detailed communications from Prof. Byamugisha and
the Permanent Secretary Ministry of Health.
Health
Call for Applications: Masters Support in Self-Management Intervention for Reducing Epilepsy Burden

-

 General2 weeks ago
General2 weeks agoApplications for Admission to Undergraduate Programmes 2026/27
-

 Agriculture & Environment5 days ago
Agriculture & Environment5 days agoTribute To Professor Abwoli Yabezi Banana (1951–2026)
-

 General5 days ago
General5 days agoSylas Ruhweza: A Brief Life Marked by Meaningful Accomplishments
-

 Health2 weeks ago
Health2 weeks agoCall for Applications: Masters Support in Self-Management Intervention for Reducing Epilepsy Burden
-

 General2 days ago
General2 days agoFreshers’ Joining Instructions 2026/2027