Health
Makerere University Launches Social Innovation in Health Initiative Community of Practice
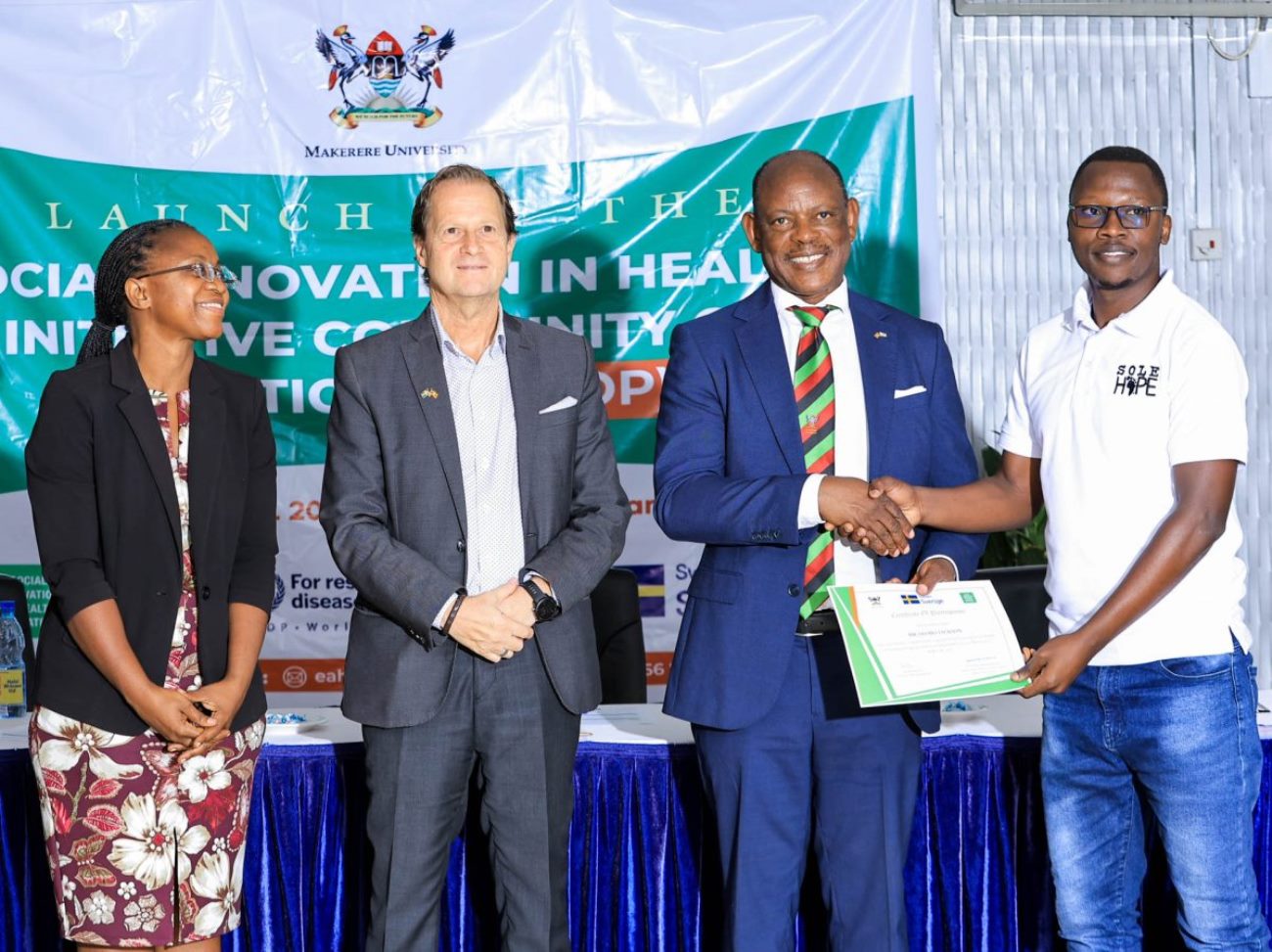
Kampala, 09 April 2025— Makerere University has officially launched the Social Innovation in Health Initiative Community of Practice (SIHICOP)—a new platform designed to connect local health innovators with policymakers, donors, and researchers. The goal: to turn scattered success stories into a powerful, nationwide movement that reimagines healthcare from the ground up.
The launch, held during the 6th National Social Innovation in Health Stakeholders’ Workshop at Hotel Africana in Kampala, drew a dynamic mix of changemakers, health innovators, academics, donors, and government leaders, all rallying around one idea: that equitable, sustainable healthcare must be rooted in communities.
While Uganda has made notable progress, cutting under-five deaths by 66% since 2000, challenges remain. Fifty out of every 1,000 children still die before their fifth birthday. Nearly half suffer from stunting due to malnutrition. In rural areas, pregnant women walk for hours to reach clinics. Across the country, hospitals battle frequent drug shortages.
Dr. Phyllis Awor, Director of the SIHI Uganda Hub at Makerere University’s School of Public Health (MakSPH), emphasized the critical role of social innovation in closing healthcare gaps. “Half of Ugandan children lack basic vaccinations, and 40% face stunting. These challenges demand creative, inclusive solutions co-created with communities,” she said.
“We’ve spent a decade identifying, studying, and strengthening grassroots innovations. Through our six-month fellowship program, we train innovators in monitoring and evaluation, research, communication, impact assessment, and fundraising so their work doesn’t just survive but scales,” she said. “Today, we’re awarding them completion certificates and launching them into a vibrant community of practice.”
Dr. Awor, who is also a Lecturer and Researcher maintains Social Innovation is about solving these real problems with real people. With the support of the Swedish Embassy and the World Health Organization’s TDR program, SIHICOP, she says, will foster peer learning, capacity-building, and scaling of innovations like mobile health platforms and community-based maternal care.

Since 2017, Uganda’s SIHI hub has supported 30 homegrown innovations, impacting tens of thousands of lives. “We’ve identified 21 standout solutions so far,” Dr. Awor shared. “But if we want them to go national, we need enabling policies.”
Globally, SIHI was founded in 2014 to bring together innovators, communities, policymakers, and academics across the Global South. With 15 hubs, including Uganda’s, SIHI has documented over 200 innovations and 40 case studies that demonstrate the power of grassroots solutions to improve health systems.
Dr. Olaro Charles, Uganda’s Acting Director General of Health Services, acknowledged that bureaucracy often stifles good ideas. “Sometimes, a small change in how you look at a problem can produce the best and most marketable solution,” he said.
He spoke from experience. As a clinician, Dr. Olaro led efforts to curb drug theft and stockouts by tightening distribution and boosting accountability. “It’s not like people walk off with whole boxes,” he explained. “But if you have 300 employees and each takes just one dose… that adds up. We introduced medicine returns, round-the-clock pharmacies, and ward-level audits. At first, there was resistance, but it worked.”
Another one of his most memorable innovations was setting up a neonatal unit for premature babies while he was a Medical Superintendent. “I remember a baby who weighed less than a kilo, barely six months old, and survived. We pushed survival rates to 85%. Eventually, we ran out of space. We began asking ourselves: Where had these children been going before? Previously, these children may have died within the community. These are innovations that create real, tangible impact. And I’m sure many of the things you’re doing here are creating similar results.”
He urged the Fellows to treat their innovations like living systems: “If they survive infant mortality, they’ll live longer. These ideas deserve to grow.”
Mr. Tomas Lundström, Health Counsellor at the Swedish Embassy, spoke with deep conviction about Sweden’s long-standing investment in Uganda’s future. “For decades, Sweden has believed in Uganda’s greatest asset, its people,” he said. “Through Sida, we funded the training of over 500 Makerere staff for PhDs. I didn’t start it. I didn’t train your PhDs. The Swedish taxpayers actually funded the training. Now that wasn’t just investment; it was transformation. It’s one reason Makerere is the powerhouse it is today.”
Lundström also shared a memory that continues to shape his view of development. While inspecting UNICEF projects in Zambia in 1998, he recalled visiting five villages where only one had shown some success. A driver suggested they visit the last village, the 5th. “We went. No one was there. We waited, then a man came running, covered in dirt. He was the village chief,” Lundström recounted. “He said something I’ve never forgotten: ‘Thomas, when the rainy season comes, we can’t take pregnant women to the clinic. Do you know where I can learn to build a bridge’?”

“That was different from what I usually hear—‘Can we have some money?’ Real change doesn’t come from handouts. It starts within communities.”
But Lundström warned that international aid is under strain. “We’ve already lost a lot of funding from U.S. and other donors. Ukraine, Sudan—global crises are pulling resources away. We must get creative. We must find new ways to secure resources.”
Still, he was optimistic. “We’re seriously considering continued support for another year. We’re also pushing for deeper collaboration between Makerere and Karolinska Institutet. But it’s up to you too,” he said.
He praised Dr. Phyllis Awor and her team: “What sets them apart is not just competence, but passion. She doesn’t do this because it’s her job; she does it because she believes in it. Because everyone deserves a fair chance, a seat at the table, a bit of hope.”
Makerere University Vice Chancellor, Professor Barnabas Nawangwe, echoed those sentiments, describing the School of Public Health as the university’s “engine of change.” He noted that the School contributes to nearly 30% of all university publications—and brings in 40% of its research funding.
“That’s no accident,” he said. “Public health is critical. Without health, there is no progress. That’s why donors invest in public health issues.”

He described the social innovation initiative as a model for how academia and communities can work together, not just to publish but to transform lives. “When global rankings name Makerere the most community-impactful university, they’re recognizing what happens when scholars step beyond lecture halls. This is what happens when researchers dig deep into the ground to cultivate solutions that transcend national boundaries.
The Vice Chancellor also paid tribute to Sweden’s role in that transformation. “We cannot thank the people of Sweden enough. Their support through Sida trained over 500 of our staff to the PhD level—the largest staff development initiative I’ve seen at any university, anywhere. It came when we needed it most, after the war. That’s why Makerere stands today as a leading research institution in Africa.”
He congratulated the 2024/25 Fellows, praising their inspiring journeys, and commended Dr. Awor and her remarkable team of researchers for achieving what only world-class institutions can: “melding razor-sharp academia with the wisdom of villages, policy muscle with frontline innovations.”












Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General6 days ago
General6 days agoUndergraduate Admission Lists 2026/2027
-
 General5 days ago
General5 days agoFreshers’ Joining Instructions 2026/2027
-
 General6 days ago
General6 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General6 days ago
General6 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General5 days ago
General5 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training