Health
Mak Researchers Partner with Safe Bangle Technologies to Roll out a Real-Time Domestic Violence Reporting Bracelet

By Joseph Odoi
A Consortium of Researchers from Makerere University School of Public Health/Resilient Africa Network (MakSPH/RAN), Medical College of Wisconsin (MCW), Somero Uganda together with Safe Bangle Technologies have rolled out a real time domestic violence reporting bracelet.
This roll out was made possible with support from the United States Agency for International Development (USAID) under the PARTNERSHIPS FOR ENHANCED ENGAGEMENT IN RESEARCH (PEER) program and the National Academies of Sciences.
Dr. Juliet Kiguli, the Principal Investigator from Makerere University, along with Dr. Roy Mayega, Deputy Chief of Party at RAN, and Dr. Agnes Nyabigambo, the study coordinator, initiated the PEER program to identify entry points for testing SafeBangle Technologies (a social enterprise based at Resilient Africa Network (RAN) with a mission to create a safer and more secure environment for women and children through innovative, affordable, and creative technology solutions to curb GBV in Africa.) wearable safety bracelet in the informal settlements. This decision stemmed from findings of increased intimate partner violence (IPV) and gender-based violence (GBV) in three informal settlements in Kampala, Uganda, following a longitudinal study, geospatial mapping, and interviews. The project, titled ‘The Impact of the COVID-19 Pandemic on Gender-Based Violence among Women and Girls in Informal Settlements in Kampala,’ highlighted the urgent need for affordable and immediate reporting mechanisms for violence.”
‘’While carrying out a study after the Covid-19 Pandemic, we identified gaps when it comes to reporting and response to Gender Based Violence (GBV) among women in informal settlements. Therefore, we used incorporated the SafeBangle intervention to solve the problem of lack of affordable and immediate reporting mechanisms for violence using a bracelet that reports violence in real time’’ explained Dr. Kiguli.
Innovation details
According to Saul Kabali and Messach Luminsa, the innovators behind SafeBangle from SafeBangle Technologies, hosted at the Resilient African Network Lab. ‘’The inspiration behind SafeBangle came from a deeply personal place. ‘’We heard countless stories of women who couldn’t call for help during moments of danger. We were deeply affected by the story of Aisha, a young woman in a rural village who was attacked while walking home alone at night. With no way to call for help, she felt helpless and vulnerable. This incident made us realize the critical need for immediate reporting alert tools, accessible to women like Aisha. We knew technology could play a crucial role and this incident awakened a strong desire in us to create a solution’’

“While developing SafeBangle, we tested with the users in both rural and urban contexts. We piloted the innovation around Kampala with support from Digital Human Righs Lab and Naguru Youth Health Network as well as it in five districts of Karamoja region with support from Save the Children and Response Innovation Lab. Right now it has become handy in Kamapala‘s informal settlements. We envision a future where SafeBangle becomes a standard tool in the fight against GBV, ensuring every woman feels safe and secure as it has the potential to transform how we respond to GBV in Africa” added Kabali.
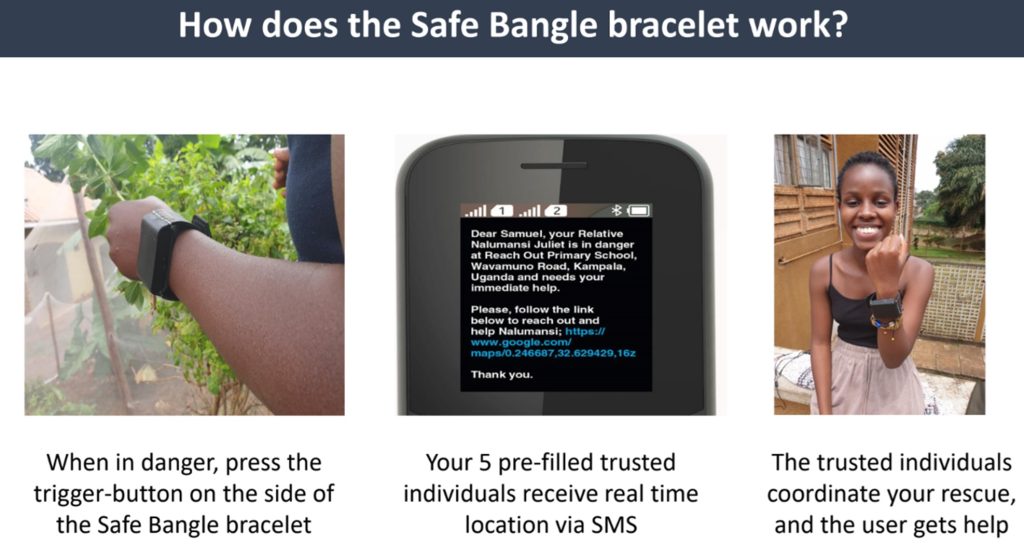
HOW THE SAFEBANGLE TECHNOLOGY WORKS
The SafeBangle is wearable technology similar to a smartwatch that sends an alarm by SMS to people chosen by a woman herself if she feels threatened.
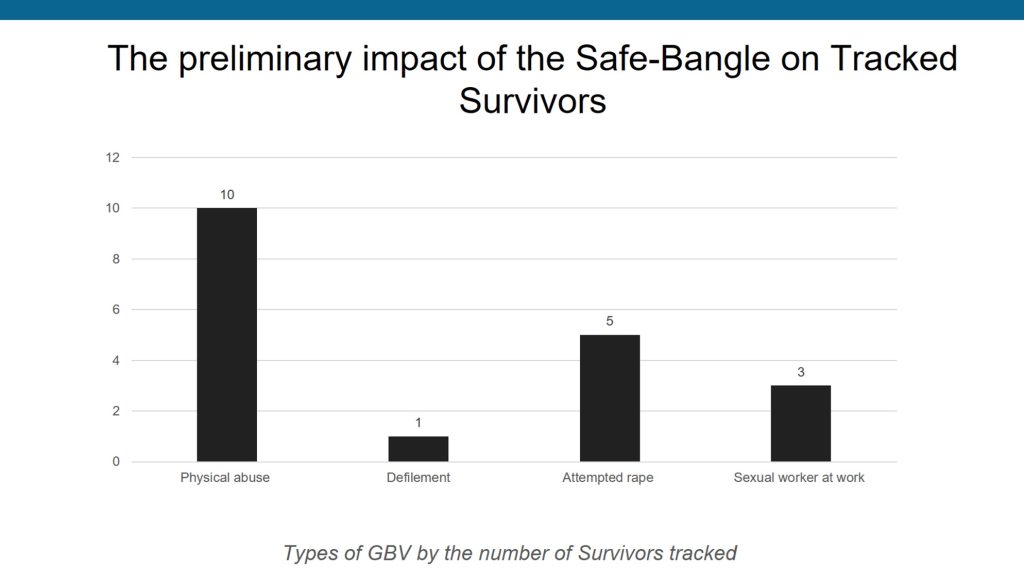
In terms of the acceptability of the SafeBangle innovation as a solution to GBV among at-risk women in informal settlements Of the 72 adolescent girls and women who received the SafeBangle, 22 activated the reporting button, resulting in 19 receiving immediate and appropriate support, including counseling, police intervention, and health services.
All adolescent girls and women who experienced GBV received a phone call from Somero Uganda to discuss the most appropriate intervention, including counseling, police cases being handled by the probation office, referral for health services, and post-exposure prophylaxis. All the GBV survivors received support and are still receiving continuous follow-up.
Researchers conducted a survey among 644 girls and women in Kinawataka (Nakawa Division) and Bwaise (Kawempe Division) to gain insights into awareness and understanding of sexual and gender-based violence among adolescent girls and women in informal settlements. The survey measured socioeconomic factors, mental health symptoms, and exposure to GBV. Focus group interviews were conducted with a separate sample of women over 18 in the settlements to explore responses to GBV.
A tabular representation of the key findings and lessons learned from your study on gender-based violence (GBV)
| Key Findings | Lessons learned |
| Prevalence of GBV. – Overall prevalence: 34.1% of women and girls reported experiencing GBV. – Among adolescents (15-19 years): Over 50% reported experiencing GBV. | – The pandemic highlighted the need for accessible and comprehensive support services for GBV survivors. – Schools emerged as crucial safe spaces for girls, emphasizing their well-being during crises. – Economic independence proved crucial, enabling women to leave abusive environments. – Involving men and boys as allies in GBV prevention efforts is essential. |
| Age-related trends | – GBV prevalence tends to decrease with increasing age. |
| Physical and health consequences. | – Women and girls suffered physical violence, injuries, and deaths, primarily from domestic violence and unsafe abortions due to limited healthcare access. – GBV resulted in unintended pregnancies, unsafe abortions, and increased risk of sexually transmitted diseases (STIs) like HIV/AIDS. |
| Social and economic impact. . | – GBV contributed to family breakups, strained marriages due to financial stress. – Economic hardships forced some women and girls into transactional sex, exposing them to further health risks and exploitation. – Pandemic-related job losses and economic constraints increased financial dependence on abusers, trapping women in violent situations. – School closures and increased household responsibilities limited women’s job opportunities and subjected them to sexual harassment. |
| Psychological effects | – Survivors experienced guilt, shame, anxiety, fear, and suicidal thoughts due to ongoing abuse. |
| Long-term effects | – Post-COVID-19, survivors faced disrupted education, early marriages, pregnancies, social stigma, and persistent mental health issues. |
Reproductive Health Consequences: GBV resulted in unintended pregnancies, unsafe abortions, and increased risk of sexually transmitted diseases (STIs) like HIV/AIDS.
Family Breakdown: The rise in GBV led to family breakups as women fled abusive relationships. Marriages were strained due to increased financial stress.
Transactional Sex for Survival: Desperate for basic needs due to job losses and economic hardship, some women and girls resorted to transactional sex, exposing them to further health risks and exploitation.
One study participant stated, “The time of COVID-19 was so terrible for some of us. We in fact got a lot of diseases from it because you would want to get food and didn’t have money. That way you would be forced to get a man who would use you and pay.” – (FGD_Girls_19–24years_Kinawataka).
Economic Effects: COVID-19 restrictions caused job losses and limited economic opportunities, particularly for women in the informal sector. This increased financial dependence on abusers and trapped women in violent situations.
Limited Access to Employment: School closures and increased household chores limited women’s ability to seek employment, perpetuating gender inequality in the workforce. Some faced sexual harassment from potential employers.
Psychological Effects: Survivors of GBV experienced guilt, shame, anxiety, fear, and even suicidal thoughts due to the constant threat and unpredictability of abuse.
Post-COVID Effects: GBV survivors faced long-term consequences, including disrupted education, early marriage, early pregnancy, social stigma, and persistent mental health issues.
Lessons learned
The pandemic highlighted the need for accessible and comprehensive support services for survivors of GBV, the significance of schools as safe spaces for girls, and the need to prioritize their well-being during crises. Economic empowerment emerged as a significant protective factor for women and girls. Those with greater economic independence were better equipped to leave abusive environments and secure their safety and well-being, while dependent ones suffered abuses. Engaging men and boys as allies in the fight against GBV and involving them in prevention efforts can help promote positive behavior change and foster more equitable relationships.
Recommendations
To address GBV against women and girls, the researchers recommend the following moving forward;
- There is need to integrate technology-driven solutions like SafeBangle into national GBV prevention and response strategies. SafeBangle can be a valuable tool for policymakers as cases of violence that would have gone unreported will be brought to light and the would-be victims will be able to get immediate help from trusted relatives and friends.
- Provide economic opportunities and vocational training for women and girls to enhance their financial independence and reduce vulnerability to violence. There is therefore a need to introduce education and training programs that empower women and girls, by providing them with skills, resources, and opportunities to start their own ventures and to participate fully in community affairs.
- Strengthen and enforce existing laws and policies related to GBV, including laws against domestic violence, child marriage, and sexual assault without discrimination be it for law enforcers, leaders, and employers where such cases were suffocated. Ensure that perpetrators are held accountable through swift and fair legal processes that have no room for corruption.
- Establish and promote effective, accessible, and confidential reporting mechanisms for GBV incidents that provide confidence and can be trusted by survivors to enhance reporting of such incidences of GBV. Community Engagement and Involvement: Involve community leaders, religious leaders, and elders in discussions about GBV to promote gender equality, change social norms, and reinforce the message that violence against women and girls is unacceptable.
- Launch extensive public awareness campaigns to challenge harmful gender norms, report cases of GBV, raise awareness about the consequences of GBV, and promote positive behaviors and attitudes towards women and girls.
- Implement comprehensive sexuality education in schools and communities, educating young people about healthy relationships, consent, and reproductive rights to be able to make informed decisions about their own lives and well-being.
- Engage men and boys as allies in the fight against GBV, encouraging them to challenge harmful masculinity norms and behaviors. This will help minimize GBV because mostly they are the perpetrators. Strengthening Support for Survivors: Provide ongoing support and follow-up services for survivors of GBV mostly counselling services to aid their recovery and facilitate their reintegration into society.
- Provide ongoing support and follow-up services for survivors of GBV, mostly counseling services to aid their recovery and facilitate their reintegration into society.
- Provide avenues to seek free or subsidized services by survivors of GBV medical services and legal processes by survivors of GBV to enhance reporting of GBV cases, access to medical care, counseling, legal support, and other essential services.
- Encourage and support more research and innovations like SafeBangle to curb incidents of GBV.
- A comprehensive and inclusive approach is required. The efforts should involve government institutions, civil society organizations, community leaders, and individuals working together to address the root causes and provide support to survivors.
- Involve media in GBV prevention activities and for enhancing campaigns against GBV mostly on radio and TV.
MORE ABOUT THE STUDY
The core project team, included researchers at Makerere University School of Public Health (MakSPH), Medical College of Wisconsin (MCW) led by Prof. Julia Dickson-Gomez, SafeBangle Technologies, and Somero Uganda, a community-focused NGO, began the project by designing their research protocol and taking a CITI Program course on human subjects social/behavioral research. Team members also met with the Ministry of Gender, Labour, and Social Development (MGLSG) in support of the gender-based violence policy process, Ministry of Health and local government. They also established relationships with the Kampala Capital City Authority (KCCA) and Nakawa and Kawempe probation offices to support legal processes for the GBV survivors. SafeBangle Team also received an award from Defenders Protection Initiative.











Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General7 days ago
General7 days agoUndergraduate Admission Lists 2026/2027
-
 General5 days ago
General5 days agoFreshers’ Joining Instructions 2026/2027
-
 General6 days ago
General6 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General7 days ago
General7 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General6 days ago
General6 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training