Health
Study Reveals Epilepsy Prevalence & Treatment Barriers in Uganda, Urgent Need for Awareness & Resources

By Davidson Ndyabahika & Julius Mugaga Tukacungurwa
A new study conducted in Uganda has unveiled the prevalence of epilepsy and identified significant barriers to treatment. The study conducted by Makerere University School of Public Health in partnership with Ministry of Health and Duke Global Neurosurgery and neurology, utilized community-based screening methods, found that urgent action is needed to increase awareness and allocate more resources to address this pressing public health issue.
Nearly 80% of individuals with epilepsy reside in low- and middle-income countries (LMICs), and a staggering 75% of those with epilepsy in LMICs do not have access to treatment. This alarming trend is further exacerbated by the stigma surrounding epilepsy, which often leads people to avoid seeking medical care due to fear of discrimination or social ostracization. The study underscores the urgent need to address the barriers to treatment, including stigma, and allocate more resources to improve epilepsy care in LMICs.
By providing a community-based descriptive statement about epilepsy in Uganda, this study sought to contribute vital information for intervention planning, addressing the urgent need for increased awareness, support, and access to treatment for people living with epilepsy in Uganda.
At the Epilepsy National Prevalence Study Dissemination and Dialogue meeting held on Wednesday, April 5, 2023 at the Golden Tulip Hotel in Kampala, Professor Anthony Fuller, the USA & Duke Neurosurgery Principal Investigator, revealed concerning findings.
The study unveiled that the national prevalence rate of epilepsy in Uganda is alarmingly high at 1.69 per cent, indicating that over 770,000 Ugandans are living with the disease. Professor Fuller’s presentation shed light on the urgent need for increased awareness, support, and intervention for those affected by epilepsy in Uganda.
During the investigation, participants were asked about their experiences with epilepsy, including symptoms such as shaking, falling, loss of consciousness, bladder control, and abnormal sensations. These questions were part of the primary screen in Phase One of the study, aimed at gathering information on epilepsy-related experiences in the past year.
With a meticulous screening process, the study examined 35,056 individuals suspected to have epilepsy, of whom 2,284 were found positive for unadjusted epilepsy, translating to a prevalence rate of 6.52% in the primary phase.
In the secondary phase, 732 individuals were confirmed positive for unadjusted epilepsy, resulting in a prevalence rate of 2.09%. In this phase, participants were asked about the frequency of attacks, occurrence in children during fever, and association with malaria-related hospitalization. These questions sought to gather additional information to aid in assessing and analyzing the nature and context of participants’ experiences with epilepsy.
Through rigorous clinical validation, including Neuro validation and electroencephalogram (EEG) tests, 594 individuals were confirmed to have epilepsy, bringing the final prevalence rate to 1.69%.
In the Central region, out of 11,746 individuals screened, 198 were confirmed positive for epilepsy, while 11,548 were negative, resulting in a prevalence rate of 1.69%. In the Eastern region, 125 out of 5,776 screened were positive, with a prevalence rate of 2.16%. In the Northern region, 68 out of 5,037 screened were positive, resulting in a prevalence rate of 1.35%. Lastly, in the Western region, 203 out of 12,497 screened were positive, with a prevalence rate of 1.62%.
These regional findings shed light on the distribution of epilepsy cases in Uganda and highlight the need for tailored interventions and support at a local level. “The epilepsy prevalence is unevenly distributed, ranging from zero to over 5% in specific districts,” says study report.
Dr. Fredrick E Makumbi, an Associate Professor and a Ugandan Principal Investigator for the study from MakSPH, highlighted the gap in community awareness regarding epilepsy treatment, leading to an increased prevalence rate.
He pointed out that the youth, aged 18 to 35, had a prevalence rate of 2.37 percent, while those aged 36 to 60 had a prevalence rate of 2.33 percent. Along with other investigators and participants, Professor Makumbi emphasized the need for further studies to identify driving factors and take equitable action.
Dr. Angelina Kakooza Mwesige, a Co-Principal Investigator for Uganda who is also a Senior Lecturer and Paediatric Neurologist in the Department of Paediatrics and Child Health, Makerere University School of Medicine noted interesting gender regional variations of epilepsy with higher prevalence in women compared to men.
In the Eastern region, the prevalence rate was higher in females at 2.40% compared to males at 1.97%. Similarly, in the Central region, the prevalence rate was 1.81% in females and 1.53% in males. In the Northern region, the prevalence rate was 1.33% in females compared to 1.37% in males, while in the Western region, it was 1.54% in females and 1.72% in males.

This revelation according to Dr. Kakooza has prompted further consideration for conducting a specialized study to investigate the underlying factors contributing to this statistic.
“We found the overall prevalence rate is 1.73% in female compared to 1.63% in male. We do not know the reason yet but we are investigating this. Also, what we found out, the medicine that can help treat this disease and the trained specialists are not enough. We need to ensure equal and free access to medicine for all. I appeal to all Ugandans, a person with this disease, just like any other disease deserves our support and care,” said Dr. Kakooza.
Dr. Daniel Kyabayinze, the Director of Public Health at the Ministry of Health -Uganda, thanked the researchers for the great study and acknowledged that epilepsy requires lifelong treatment and highlighted the need to continuously provide treatment for all those affected.
According to Dr. Kyabayinze, the government plans to use the study’s findings to estimate the treatment needs, and Kyabayinze expressed confidence that further examination by Makerere University School of Public Health’s partners will help identify associated factors, such as potential agents or organisms, that can be modified to combat epilepsy. He also noted that while some individuals are already receiving treatment, many Ugandans face challenges in affording the necessary treatment for epilepsy.
Dr. Kyabayinze emphasized the importance of placing mental health specialists in various locations across the country to ensure access to services, stating, “There is also a need to intensify sensitization efforts to avoid stigmatizing people with epilepsy and ensure they receive the services they need.”

Ms. Nina Mago, Founder and Program Advisor of Purple Bench Initiative, underscores the need policy makers to prioritize healthcare needs of individuals with epilepsy to needs of people with epilepsy. She emphasizes affordable access to good quality medication.
“When you have medication, you have less seizures and you become more confident on being independent, to participate in activities which may include going to school, holding up a job, social interaction but all this is possible when there is also strong awareness,” says Nina.
Ms. Mago, says epilepsy is a life-threatening condition; “I came up with a connotation of a phone battery, as a notification of battery low shows up, equally relates to a life about to be lost.”
Dr. Olaro Charles, the Director Health services – Clinical in the Ministry of Health stated that epilepsy remains one of the common mental health conditions in Uganda. He said that they have just concluded a joint review mission and found out that from all their mental health facilities, epilepsy constitute to almost 55.4% of patients.
“If you look at 2019/2020 they were about 314,000 then came to about 340,000 and then last year it was 251,000. This mapping however is very important because it helps us to plan for care. If we do the same in those regions with high prevalence, we may be able to plan well”. Dr. Oralo.
Dr. Sarah Nekesa, Executive Director of Epilepsy Support Association Uganda, called on members of Parliament to increase the budget for mental health drugs, including epilepsy medication, and ensure their availability. She emphasized the need for integrating epilepsy services with other healthcare services to improve accessibility.
Additionally, Dr. Nekesa highlighted the importance of grassroots awareness to combat stigma, and urged the government to allocate adequate human resources and support from health workers to encourage peer talks and build confidence among people living with epilepsy.
“We should increase the drug availability in health facilities and make sure that a person with epilepsy is able to get medication whenever they need it. Epilepsy is not understood by everyone so if everybody understands epilepsy it would be easier for treatment and stigma to go down and integration of epilepsy in every service that is given to the community”. Said Dr. Nekesa.












Fifteen years after a sustained investment of over $100 million, Makerere University has transitioned Uganda’s digital health systems and assets to the Ministry of Health, marking a fundamental shift from externally supported interventions to full national ownership.
On 31 March 2026, a handover ceremony at Uganda’s Ministry of Health marked the closing of one chapter in Uganda’s digital health journey and the beginning of another, one in which systems built over 15 years through the Makerere University School of Public Health Monitoring and Evaluation Technical Support (MakSPH-METS) Program now sit firmly within government hands.
The national handover event brought together a cross-section of Uganda’s health leadership, academia, and development partners, led by the U.S. Ambassador to Uganda, H.E. William W. Popp; the Permanent Secretary, Dr. Diana Atwine; and the Director General of Health Services, Dr. Charles Olaro. They were joined by the CDC Country Director, Dr. Mary A. Boyd, senior government officials, implementing and development partners, technical teams, and the media. At the center of that moment was Makerere University School of Public Health, an institution that, over more than 70 years, has built its reputation as one of the region’s most enduring public health research and training hubs, working hand in hand with ministries of health, districts, referral hospitals, and partners to turn evidence into public systems that last.


Back in time, Uganda had made important gains in HIV control, but behind those gains were structural weaknesses that could not be ignored: fragmented data monitoring and evaluation systems, parallel reporting channels, weak digital integration, limited surveillance responsiveness, constrained oversight in decentralized structures, and uneven quality assurance across the HIV continuum of care. The problem was not simply that data existed in too many places but it was that the health system could not always use that data quickly enough, coherently enough, or at sufficient scale to guide action.
The MakSPH-METS program was designed as a response to that reality, build the backbone of a data-driven health system, supported through three successive grants totaling US$103.8 million by the United States Government through Centers for Disease Control and Prevention (CDC) and the President’s Emergency Plan for AIDS Relief (PEPFAR).
The program, rather than working around government systems, worked inside them with a deliberate and system-wide focus to strengthen health information systems, expand surveillance, improve governance and accountability, institutionalize quality improvement, and build the workforce needed to run all of it.
That choice to work within the Ministry of Health structures and across decentralized systems made all the difference. It meant the investment was not in parallel projects, but in national architecture, and over time, that architecture began to take shape.

Reporting through DHIS2 (District Health Information System 2), the world’s largest open-source health management information system platform improved from 58 percent in 2020 to 98 percent in 2025. DHIS2 is a flexible, web-based tool used to collect, manage, and analyze both aggregate and individual-level data.
Also, tracked through the MakSPH-METS program, electronic medical record coverage rose to a high of 86 percent in 2024 from 50 percent in 2020, and reached 100 percent in high-volume sites. Additionally, a functional National Data Warehouse came into place. Across the country, 1,300 health facilities implemented HIV case-based surveillance, 1,084 facilities implemented HIV recency surveillance, and 300 sites established all-cause mortality surveillance. Six regional referral hospitals were implementing integrated surveillance for severe acute respiratory infections, influenza-like illness, acute febrile illness, and SARS, popular for Severe Acute Respiratory Syndrome, which is a viral respiratory illness caused by the SARS-associated coronavirus. At the governance level, 10 regional referral hospitals and 65 CDC-supported districts were trained and supported in planning and oversight, while regional referral hospital capacity scores improved from 58 percent in 2021 to 79 percent in 2024.
These are strong statistics. But the deeper story is that Uganda moved from fragmented systems to a more integrated, data-driven public health response. What had once been separate reporting streams, paper-heavy workflows, and delayed visibility became a system able to provide more timely access to data, better accuracy, stronger dashboards, and more confident decision-making. Health workers could access patient information faster. Today, district leaders are able to review performance data more accurately, national programmes can respond more strategically and data is no longer just collected, but used.
The transition also touched the practical side of care, including laboratory systems, patient records, commodity tracking, quality improvement, and outbreak intelligence.
Dr. Alice Namale, Executive Director of MakSPH-METS Program, was careful during the handover not to let the digital systems overshadow the broader institutional gains. MakSPH-METS, she noted, had “improved regional referral capacity and the district health team capacity to manage programs,” and those systems were now being leveraged by disease programs beyond HIV. She also captured the spirit of the team behind the work, saying the staff had adapted through a changing landscape. “For us, it was never business as usual. We had to continuously adapt as the landscape kept changing, and the team delivered with grace and professionalism,” Dr. Namale said.

Adding that; “We have strengthened systems and built capacity across the health sector, and these gains are now supporting not just HIV programs, but broader health services.”
That wider view matters that the systems handed over were not only about HIV reporting but they included platforms for electronic medical records, HIV case-based surveillance, stock monitoring, quality improvement, early infant diagnosis, viral load reporting, PEPFAR reporting, DREAMS tracking tool for tracking adolescents and young people data, outbreak and respiratory illness surveillance, ICT asset tracking, and e-learning platforms. In plain terms, these are the tools that allow clinicians to see results faster, managers to monitor performance more clearly, districts to respond to outbreaks sooner, and national leaders to plan with greater confidence.
The Ministry of Health now boasts of 16 such systems that have been fully developed and handed over, including UgandaEMR repositories, DREAMS Tracker, PREV Tracker, the HIV CBS dashboard, the Weekly Stock Status System, OpenHIM for health information exchange, EMR metrics, eIDSR, a platform for documenting patient level data on acute illnesses like pandemics, the QI database for visualising facility data on continuous improvement, EID and viral load dashboards, TB eCBSS, PIRS that supports PEPFAR indicator reporting beyond the DHIS2, and the SURGE Dashboard, a power BI based reporting platform.
This handover included 725 servers, more than 4,700 computing devices, solar systems for nearly 800 facilities, connectivity equipment for more than 1,300 sites, video conferencing systems, and network upgrades for regional referral hospitals. Those investments, valued at about US$9.3 million in ICT infrastructure alone, helped kick-start Uganda’s digitalization journey in practical terms: power, devices, connectivity, storage, and the ability to sustain real-time data exchange across facilities.
For the Ministry of Health, the significance of this transition is both strategic and immediate. Dr. Charles Olaro, Director General of Health Services, put it plainly that “Data is the lifeblood of decision-making,” and it provides “the raw materials for accountability.” In a sector where financing, human resources, commodities, and performance all depend on credible information, that was not a ceremonial line, but was a statement of what national ownership now requires.

“As a Ministry, we are focused on how this can support sustainable national ownership that is built to last, while strengthening resilient health systems. We look forward to leveraging these gains as part of our national digitalization roadmap, ensuring they continue to support and improve our systems moving forward,” said Dr. Olaro.
Dr. Diana Atwine, Permanent Secretary at the country’s Ministry of Health, spoke with equal clarity about what comes next. She described the handover as both a celebration of “tangible milestones of growth” and a call to responsibility. Uganda, she said, is not going back to paper-heavy systems. “We are not going to start again. We are just moving ahead.” At the same time, she was firm that ownership must come with inventory, verification, deployment, maintenance, and continued investment in people.

Calling the digital systems and assets “this treasure,” she urged districts and hospitals to take care of it, and made a broader plea that Uganda government should not lose the skilled workforce developed through the partnership, especially the technical teams that established these systems under the program. “This is the cream of the cream,” she said, arguing that the country should find ways to retain this talent as digital systems expand.

On his part, the U.S. Ambassador to Uganda, William W. Popp, framed the handover in similar terms, as a move from project implementation to self-reliance. He described it as “a new phase in national ownership and sustained self-reliance,” and linked it to the December 2025 U.S.-Uganda health memorandum of understanding, which set out a broader vision of government-led delivery, accountability, and stronger national systems. He stressed that foreign assistance, when delivered with discipline and accountability, should build lasting national capacity. In his words, the handover symbolizes a stronger Ugandan health system that benefits Uganda, the region, and the wider world.

For Makerere University School of Public Health, the moment was deeply consistent with its long institutional identity. The School began in the 1950s as preventive medicine, grew into one of sub-Saharan Africa’s earliest public health institutions, and has remained closely linked to the Ministry of Health through teaching, service, research, and workforce development.
Emphasizing the Ministry’s continued reliance on national expertise and long-standing institutional partnerships, the Permanent Secretary underscored the critical role of the Makerere University School of Public Health in sustaining and advancing Uganda’s health systems:
“We are still going to work with you… because you are our important resource in the country. You have the skill, you have the experience—and above all, you are Ugandans,” Dr. Diana Atwine said emphatically.

Her remarks stresses not only MakSPH’s technical capacity, but also the trust it has built over years of collaboration with government positioning the School of Public Health as the Ministry of Health’s strategic partner in driving nationally owned, sustainable health system improvements.
MakSPH has worked across more than 25 countries in Africa in recent years, trained thousands of public health professionals, and sustained long-term partnerships with organizations including CDC, NIH, the Global Fund, Johns Hopkins, WHO, the UN agencies and others. Its own strategic direction emphasizes community engagement, policy influence, partnership, and translating research into practical public good.
That is why Prof. Rhoda Wanyenze, Dean of MakSPH and Principal Investigator of METS, described the handover not as an ending, but as a transition. “As an academic institution, we are always exploring—looking for innovative, creative ways of doing things. We test them, and then work with key actors to take them over, scale them up, and sustain them,” she said. Later, she added, “This is not the end. This is the beginning of a new phase.”

For Wanyenze, that philosophy has always been intentional. “This is not our data, this is not our house, this is Ministry of Health,” she emphasized, an approach that places national ownership at the center from the very beginning. The School’s role, then, is not to hold systems, but to build them, prove them, and let them go when they are ready to stand.
And when that happens, she argues, it is not a loss but success. “When what we have contributed to is taken over, sustained, and continues to grow—that is success.”





For years, much of Uganda’s health system operated with limited visibility, records stacked in paper files, data delayed, and decisions often made without a clear picture of what was happening on the ground. That is what makes this moment different.
After more than 15 years of investment and collaboration, Uganda is now taking over a digital health infrastructure built not just to collect data, but to actually use it, making information more timely, accessible, and practical for decision-making. The handover of the Monitoring and Evaluation Technical Support (MakSPH-METS) programme assets and systems marks more than a transfer of equipment or platforms; it reflects a shift toward a system that can better generate and use its own data.
In the end, the legacy of MakSPH-METS is not only the hardware, but something less visible and more important: a stronger ability to make informed decisions, knowing where the burden lies, where gaps remain, where stockouts occur, where patients are lost, and where progress is being made.







In Uganda, children arrive at health facilities every day with fever, cough, injuries or routine illnesses. What health workers rarely recognise is that some of these children are already living with alcohol or other substance use disorders, conditions that complicate diagnosis, delay treatment, and quietly undermine children’s health, development, and long-term wellbeing.
This hidden reality was uncovered by Dr. Harriet Aber Odonga during her doctoral research at Makerere University School of Public Health (MakSPH). Her PhD study, titled “Substance Use among Children in Mbale, Uganda: Health System Landscape and Support Structures,” examined how Uganda’s health system detects and responds to substance use among children aged six to 17 years.
The findings revealed a problem far more widespread than many health workers and caregivers assumed. Nearly one in four children attending health facilities showed signs of alcohol or other substance use problems, with alcohol the most common substance. In the study, a child was classified as having a “probable” substance use disorder when responses to a standard screening questionnaire indicated harmful or dependent patterns of use requiring further clinical assessment.

The discovery adds urgency to an already serious public health challenge. Globally, alcohol and other substance use is responsible for one in five deaths and contributes to more than 200 disease and injury conditions, according to WHO. Across Africa, alcohol alone accounts for 6.4 per cent of all deaths and 4.7 per cent of disability-adjusted life years. In Uganda, alcohol use disorder affects roughly 7.1 per cent of the population and contributes to about 7% of all deaths, while research among young people shows that alcohol exposure often begins early in life.
Despite these risks, most policy and research attention has historically focused on adults and older adolescents. Much less is known about children who begin experimenting with alcohol and other substances earlier in their childhood, a gap Aber set out to examine by studying how Uganda’s health system identifies and responds to substance use among children.

A research question begins
Aber’s interest in the subject began unexpectedly. “I remember seeing a notice calling for PhD students to research child alcohol use,” Dr. Aber recounted. “The phrase struck me immediately. I could not believe that children were drinking alcohol. That moment sparked my curiosity, so I began reviewing the literature on the subject in Uganda. During that search, I came across a study documenting alcohol use among children as young as five years old. That finding was deeply unsettling and raised many questions for me.”
With a longstanding interest in child health, Aber saw the research as an opportunity to investigate a problem that had received little systematic attention. What began as disbelief developed into a doctoral investigation examining how Uganda’s health system identifies and responds to substance use among children. She began her doctoral studies in 2021 at MakSPH under the supervision of Dr. Juliet N. Babirye, Prof. Fred Nuwaha, and Prof. Ingunn Marie S. Engebretsen from the University of Bergen, Norway. She defended her thesis on October 25, 2025, before graduating during Makerere University’s 76th graduation ceremony on February 25, 2026.

Investigating the health system response
Aber’s study examined four key questions. It measured how common substance use disorders are among children visiting health facilities. It assessed whether health facilities are equipped to screen and manage these cases. It evaluated whether screening tools are acceptable to children, caregivers, and health workers. It also examined how families seek help when children begin using substances.
To answer these questions, the research used a mixed-methods design combining quantitative surveys and qualitative interviews. Aber collected data from 834 children attending health facilities in Mbale District, assessed 54 health facilities in the district to determine their readiness to screen and manage substance use disorders, and interviewed health workers, caregivers, and children to understand experiences of care and barriers to seeking help. Additional surveys involving 602 children and 355 caregivers examined help-seeking patterns and support structures.
Quantitative data were analysed to estimate prevalence and identify associated risk factors, while qualitative interviews provided insight into how families, communities and health workers respond when children begin using substances.
What the research found

Data collected between 2023 and 2024 across health facilities in Mbale District in Eastern Uganda showed that substance use among children was far more common than many health workers and caregivers assumed. Alcohol use disorder emerged as the most prevalent form of substance use disorder among children in the study. The analysis also showed that children were significantly more likely to use substances if they were exposed to peer or sibling use, lived in lower-income households, or experienced strained relationships with caregivers.
The research also revealed major health system gaps. Only 19 of the 54 health facilities assessed, representing 35 per cent, met the minimum readiness criteria required to screen, diagnose or manage substance use disorders. Many facilities lacked trained staff, standardised screening guidelines, and clear referral pathways for specialised care.
Aber explained that substance use often goes undetected because it is rarely the primary reason children visit health facilities. “Substance use is hidden,” she asserted, reflecting on evidence from her doctoral study. “While health workers are treating other illnesses, some children coming to these facilities are already struggling with alcohol or other substances.”
She added that early substance use can have lasting consequences for children’s development. “Risk was higher among children exposed to peer or sibling substance use, lower household income, lower caregiver education, and strained child-caregiver relationships. The public should be concerned because early substance use affects brain development, mental health, education completion, and long-term well-being.”
Families often navigate the problem alone

Her research also examined how families and communities respond when children begin using substances. She found formal help-seeking to be rare. Many caregivers relied on informal networks, including relatives, teachers, religious leaders, and local authorities. Health services were seldom the first point of support.
Meanwhile, punitive responses such as discipline or punishment were sometimes used by caregivers attempting to stop the behaviour of substance use among children, but these responses rarely addressed the broader social and family pressures influencing the vice.
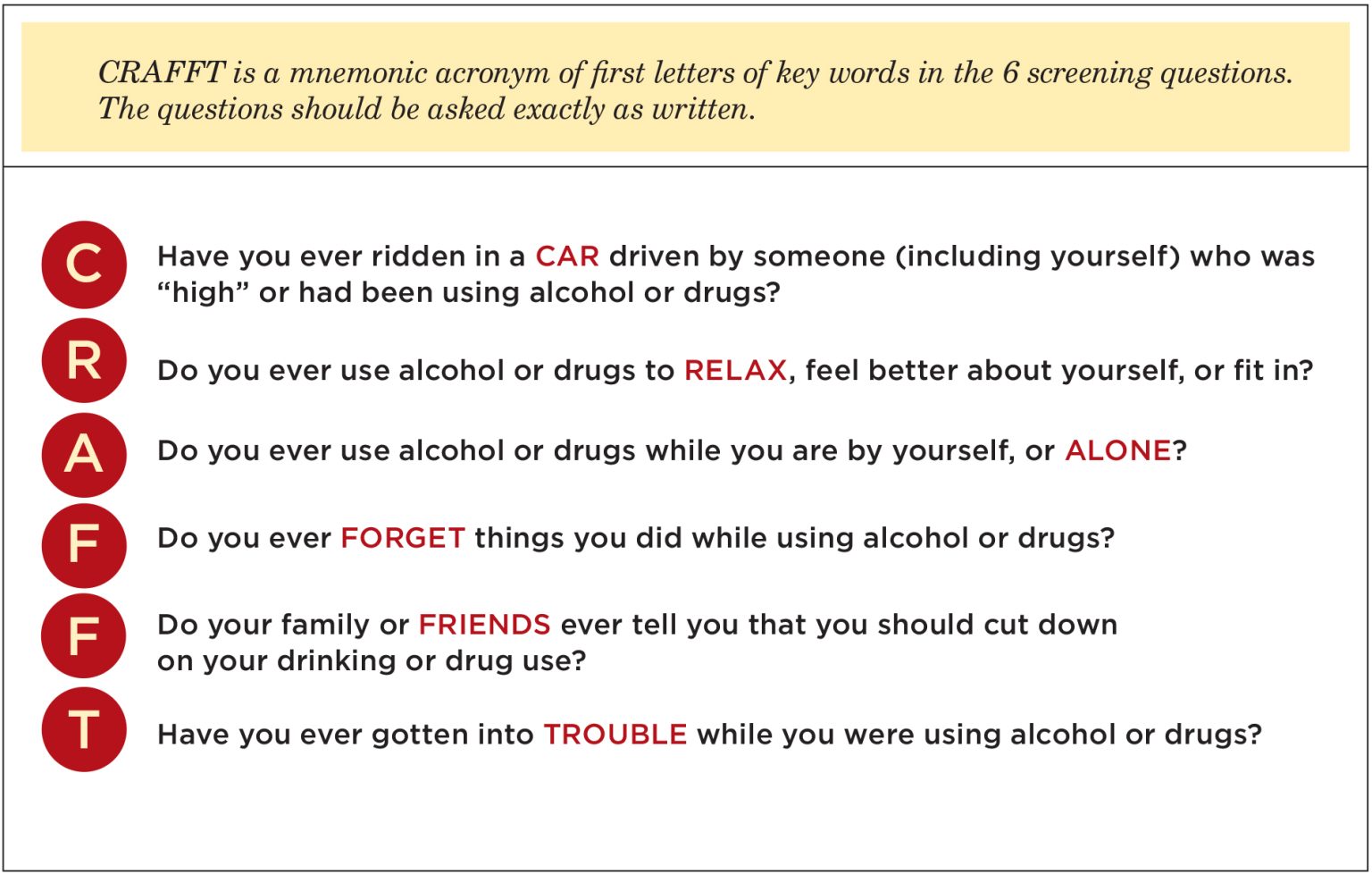
One encouraging finding emerged from her study’s assessment of early detection tools. Aber evaluated the use of the CRAFFT screening tool, a short set of structured questions used by health workers to identify whether a child may be using alcohol or other substances. Children, caregivers, and health workers generally found the questions from the tool easy to understand and acceptable to use. In the study, over 85 per cent of children reported the questions were easy to answer, and nearly nine in ten caregivers were comfortable with the screening process.
These findings, however, suggest that routine early detection could be integrated into primary healthcare within the communities. “If policymakers were to act on one finding from my research, I would prioritise integrating routine, age-appropriate substance use screening into primary healthcare,” Aber argued. “With proper training and referral systems, health workers can identify early risk and support children before the problem escalates.”
Training across nutrition, public health and health systems
Aber’s approach to the problem reflects a research journey shaped by training across multiple areas of child and public health. She first studied Food Science and Technology at Kyambogo University, graduating in 2011, before specialising in Nutrition during her Master of Public Health at Makerere University, graduating in 2015, before embarking on her doctoral training in Public Health at the School, completing in 2025 to graduate at Makerere University 76th Congregation.

Before beginning her PhD, she worked on nutrition research and later coordinated studies examining climate risks, anticipatory humanitarian action and community health systems. This background shaped how she approached substance use among children, not as an isolated behavioural problem but as an issue influenced by broader health and social conditions.
“I do not see child substance use as a problem with a single cause,” she noted. “It is influenced by biological, psychological, social, and system-level factors. My nutrition training helped me appreciate how substance use intersects with broader child health concerns such as mental health, family stress, and even food insecurity.” These pressures are visible in her research site in Mbale, where environmental shocks, economic hardship, and family instability persistently shape daily life. Recurrent landslides and livelihood disruptions place strain on households, and adolescents facing stress or instability may turn to substances as a coping mechanism, she holds.
From evidence to solutions
Completing her PhD has now shifted Aber’s perspective from documenting problems to identifying solutions for social impact. “Completing my PhD shifted my perspective from simply generating evidence to actively providing solutions,” she observed. “Child health challenges such as substance use, nutrition, and climate-related risks are interconnected. As a researcher, I have become more systems-focused, and as an advocate, I feel a stronger responsibility to ensure evidence informs policies that improve children’s wellbeing.”

For Aber, that responsibility extends to the families whose experiences informed the research. Parents, teachers, and health workers often notice behavioural changes first, even when they feel unprepared to respond. Listening without judgment, recognising warning signs, and linking children to appropriate support can make a significant difference, she noted, especially in a context where formal services remain limited.
Her research ultimately sends a clear message for Uganda’s health system. Children affected by substance use are already present in communities and health facilities. Detecting the problem earlier, strengthening screening systems, and equipping frontline health workers with appropriate tools could significantly improve outcomes for vulnerable children.
Behind the research journey stood a wide network of support, including MakSPH supervisors and doctoral committee, the TREAT consortium, the MakSPH PhD forum, the Health Development Centre secretariat, study participants, research assistants, family and friends, and funding support from the Government of Uganda through the Makerere University Research and Innovations Fund (MAKRIF) and the Norwegian Research Council, all of whom she remains grateful.
Aber’s research ultimately points to a critical gap in Uganda’s health system. Children affected by substance use are already present but remain largely invisible. Without routine screening, trained health workers, and clear referral systems, opportunities for early intervention are often missed. Addressing this gap, as indicated by her study, goes beyond clinical care. It requires strengthening how the health system recognises and responds to emerging risks that affect children’s long-term health and development.
By Carol Kasujja and Zaam Ssali
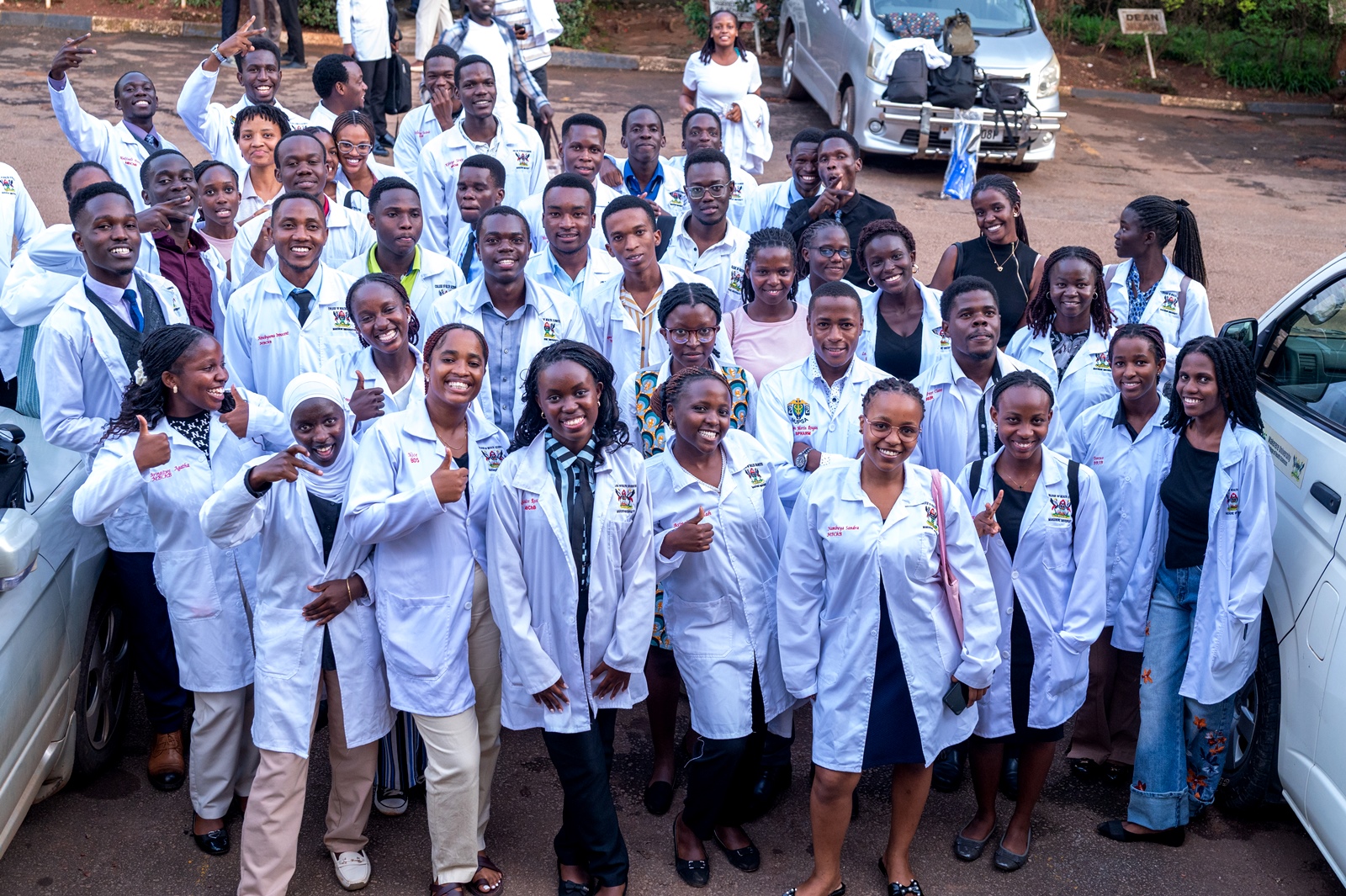
Medical students at Makerere University have been urged to wear the white coat with humility as they begin their journey in the medical profession.
The call was made during the White Coat Ceremony held on Thursday at the Makerere University College of Health Sciences in Mulago.
The White Coat Ceremony marks the beginning of a new journey in healthcare and symbolises professionalism, compassion and excellence. It represents not only the mastery of medical knowledge but also a promise to always place patients at the centre of care. It is a commitment to listen, advocate, heal, and treat every individual with dignity and respect.
“We would have given you a suit, but the symbol of the white coat reminds you that you are here to work. White signifies purity in service. You are in medical school because you are among the best, and you have some of the best lecturers,” said Bruce Kirenga, the Principal of the College of Health Sciences.

Prof Kirenga lauded the students for their dedication to a path dedicated to preserving lives and urged the students to serve with dedication and protect the image of health workers.
“These days, you can use Artificial Intelligence to generate entire coursework, but when it comes to practice, remember the university has an AI policy and you must use it responsibly. In medicine, you take responsibility for your decisions. AI may make life easier, but you must learn and use your hands. Go where the patients are,” he noted.
Prof Kirenga also reminded the students that a medical career offers different paths, including research, teaching, clinical care, and administration.
“As first-year medical students, support each other. Find peers to share your struggles with, especially those in your year. Get mentors and coaches. It took me 26 years to become a Principal, so find mentors who can guide you,” he advised.

Speaking at the event, Sabrina Kitaka, a senior lecturer at the medical school, urged students to uphold the values expected of someone putting on the white coat by being humble and making sure that they connect with their patients.
“Wearing a white coat is a symbol of your commitment to a profession full of honour. This moment is like a rite of passage, from adolescence into adulthood. Joining this noble profession does not make you more important than other students. Be humble,” Dr Kitaka said.
She also encouraged the students to show kindness and compassion to their patients.
Addressing the students, Dr Idro Richard, the Deputy Principal at the College of Health Sciences, called upon the students to always make sure that they keep patients secrets.

“People will come to you and share secrets they have never shared even with their closest family members, do not share people’s pains. If one of you makes a mistake the public will blame all the fraternity so handle your patients with dignity. Always place yourself in the life of those patients when you are in the ward,” Dr Idro, said.
Dr Idro reminded the students to always think of their safety while on the ward by avoiding open shoes.
“Be smart for your own safety, always wear closed shoes, a needle can fall and hurt your legs when you are wearing open shoes. Maintain the excellence you had when you joined and avoid doing life alone,” Dr Idro said.
He further advised the students to always create time and have fun because it is not all about medicine

“Have an open mind, have some fun and also learn other things like soft skills, write, sell and travel. You are in the best School with the best teachers do not allow mediocrity. Avoid cheating, laziness, drugs and betting,” Dr Idro, noted.
In her speech, Anne Atukunda Ronaldine, the chairperson of the Makerere University Medical Students Association (MUMSA), told the first years that they are privileged to join the College as it celebrates a century of excellence.
“Be your brother’s keeper. You will make it together if you work together as a class. Do not avoid your lectures. Medical school is a lot of work, but it gives back,” Atukunda said.

During the ceremony, the College of Health Sciences safeguarding and inclusion champions encouraged students to speak up and report any form of harassment, abuse, or unsafe situations, noting that safeguarding is everyone’s responsibility.
The champions reminded students that creating a safe learning environment requires respect for one another, responsible behavior, and the courage to raise concerns when something is not right. They also urged the new students to support their peers and make use of the available safeguarding channels whenever they feel unsafe or witness misconduct.
The Champions also called upon their peers to support students with disabilities so that no one is left behind. It was a proud moment for many first-year students to finally see themselves wearing white coats, as it was a dream come true for many. The event concluded with a cake-cutting ceremony and a dinner.
-

 General7 days ago
General7 days agoApplication for Admission to Graduate Programmes 2026/27
-

 General2 weeks ago
General2 weeks agoCustodians and Wardens trained on Fire prevention in Halls of Residence
-

 Education2 weeks ago
Education2 weeks agoMakerere University Charts New Future with the unveiling of the Open, Distance and E‑Learning Building and Strategic Plan
-

 General5 days ago
General5 days agoMastercard Foundation Scholars Program at Makerere University Celebrates the Last Cohort of Phase One Graduates
-
 General1 week ago
General1 week agoCelebrating a Life of Loyal and Distinguished Service