Research
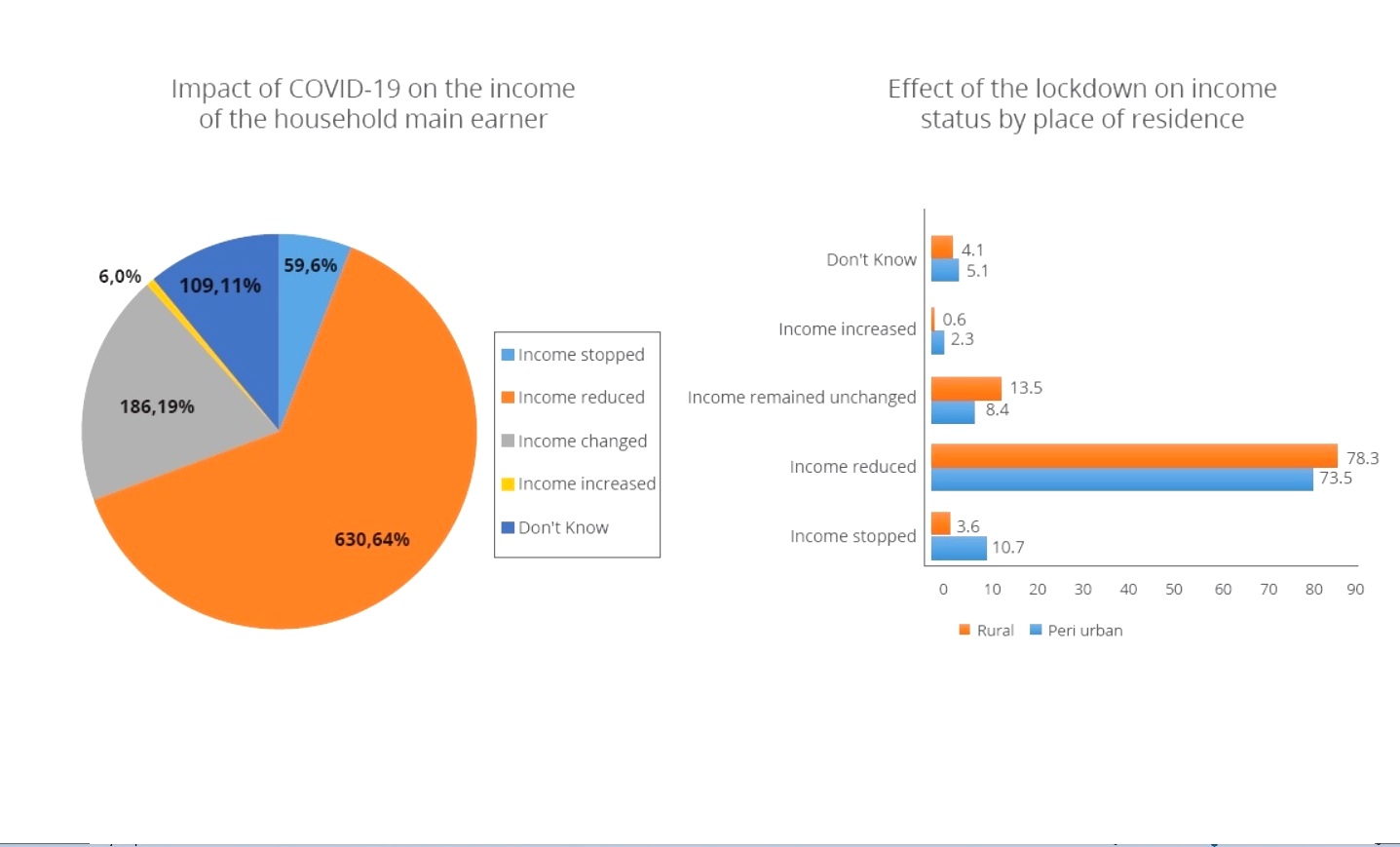
The 2020 COVID-19 Non-Pharmaceutical Containment Measures – Adherence and Impact on Livelihoods in Rural Uganda













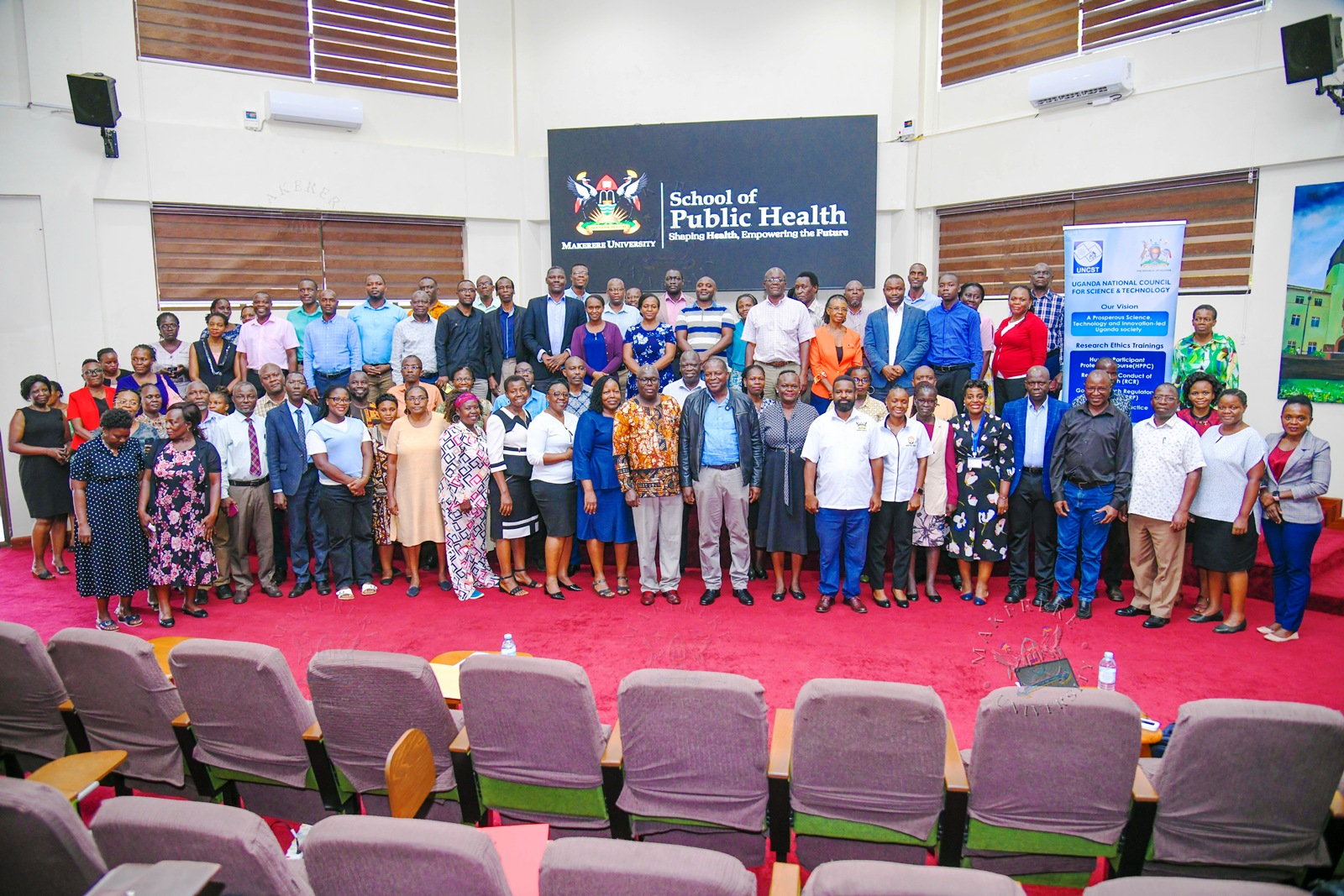
The Uganda National Council for Science and Technology (UNCST) on 24th July 2026 accredited over 90 Senior Academic Members of staff that form Makerere University‘s Research Ethics Committees (RECs) in Good Research Review Practice (GRRP) after an intensive three-day Training. The closing ceremony was presided over by the Deputy Vice Chancellor (Academic Affairs)-DVCAA Prof. Sarah Ssali who was represented by the Principal, College of Computing and Information Sciences (CoCIS), Prof. Tonny Oyana.
UNCST’s Role Appreciated
In his remarks, Prof. Oyana reiterated the core function that research plays in Makerere University‘s mission and noted that excellence in research must always be underpinned by excellence in research ethics. “Research Ethics Committees play a vital role in fulfilling this responsibility,” he stated.
“Your decisions influence not only the quality and credibility of research conducted at the University but also the trust that research participants, communities, funding agencies, policymakers, and the public place in our institution,” remarked the DVCAA, who underscored the pivotal role of RECs in upholding Makerere University‘s reputation as a centre of research excellence.

He therefore thanked UNCST for promoting responsible conduct of research and strengthening ethical review systems in Uganda through facilitating trainings for RECs in GRRP and other critical areas such as Good Clinical Practice (GCP). He equally commended the Directorate of Research, Innovation and Partnerships (DRIP) led by Prof. Robert Wamala for organising the training, which continues to strengthen research governance structures across the University.
Incorporate RECs in Governance Structures
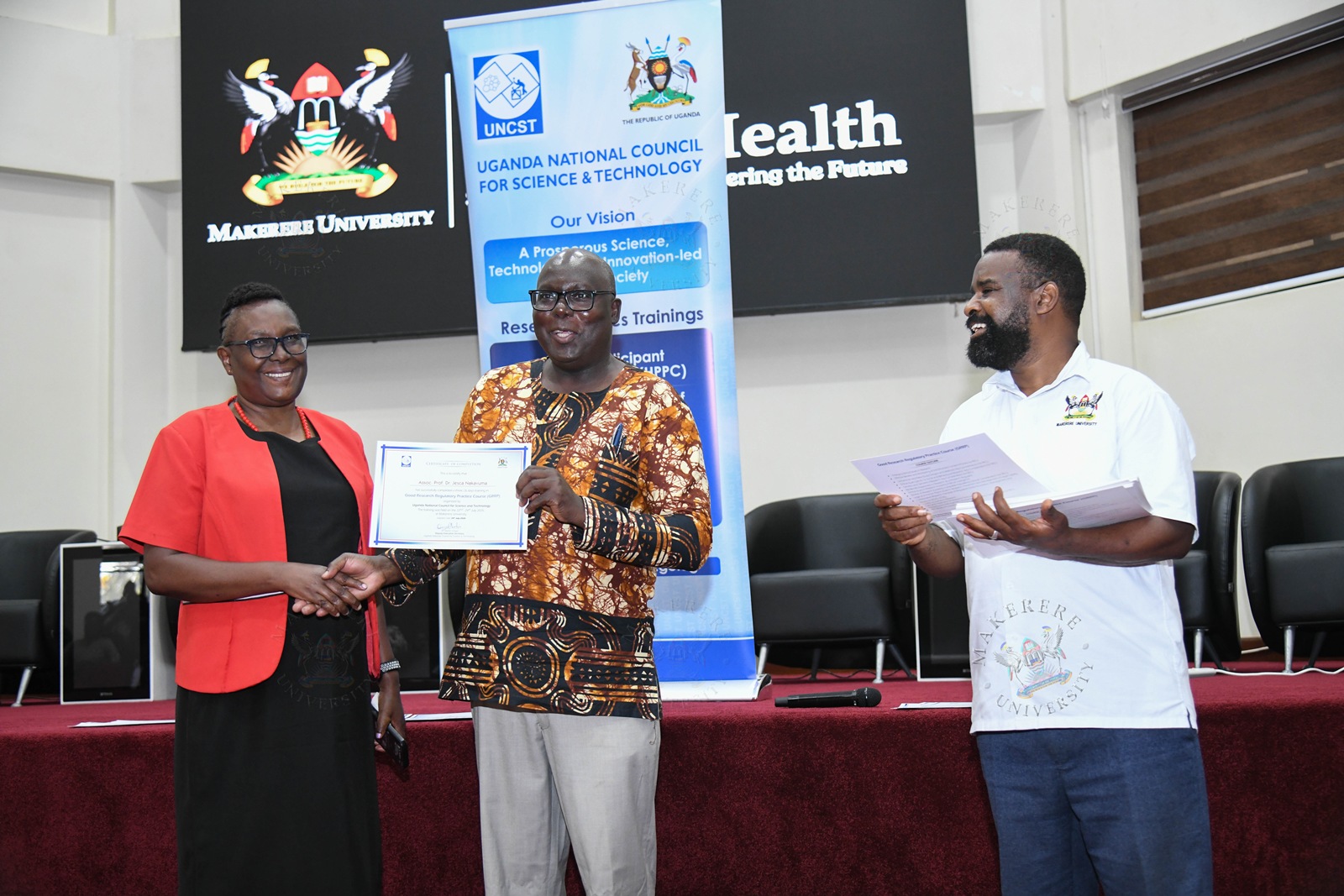
Presiding over the certificate award ceremony, the Deputy Executive Secretary UNCST, Dr. Martin Patrick Ongol congratulated all participants upon braving the three days of training despite their busy academic and research schedules. He equally commended Prof. Robert Wamala for ensuring that RECs at Makerere receive regular training and accreditation as mandated by governing procedures.

In the same breath he noted that RECs are key to ensuring that institutions conduct credible research and therefore ought not to be kept at the periphery of governance. “We would like to see that Research Ethics Committees get incorporated into governance and management structures of Makerere University – not like ad-hoc or adjunct entities within the ecosystem.”
Dr. Ongol equally called upon researchers and proposal writers in the room to ensure that issues of ethics are adequately budgeted for in the studies. “When it comes to participant compensation, we sometimes hit a snag,” he cited. He equally called upon members of RECs to ensure that issues of documentation are adequately addressed. “80% of noncompliance issues observed by UNCST are due to improper, missing or poorly handled documentation, and one of the ways of improving is through continuous engagement and we hope that we shall get there” he added.
DRIP and National Accreditation Committee Laud RECs
Prof. Robert Wamala whose Directorate of Research, Innovation and Partnerships is at the heart of coordinating training with UNCST commended members of RECs, many of whom hold the ranks of Professors, Associate Professors and Senior Lecturers for sacrificing time to complete the GRRP Training. He reiterated that RECs are at the heart of ensuring that Makerere‘s research, particularly that involving human participants, meets national and international standards through harmonised ethical review approaches.
Adding her voice, Prof. Sylvia Angubua Baluka, a member of the UNCST National Accreditation Committee noted that in addition to RECs, Institutional Animal Care and Use Committees play an important role in safeguarding the lives of animals that we depend on for food.
“I would therefore like to appreciate all Chairpersons and Members of Committees that are here; you are doing a good job and based on our site monitoring visits, we can address gaps in monitoring the research protocols you approve so as to have more impactful work and outputs that are more compliant with the ethical approval given” she added.

RECs at a glance
A total of 95 members of RECs took part in the GRRP Training as broken down below.
- Makerere University School of Medicine Research Ethics Committee (SOM–REC) – 19
- Makerere University School of Biomedical Sciences Research Ethics Committee (SBS–REC) – 17
- Makerere University School of Health Sciences (SHS–REC) – 15
- Makerere University School of Social Sciences Research Ethics Committee (MakSS–REC) – 5
- Makerere University School of Public Health Research Ethics Committee (MakSPH–REC) – 19
- Makerere University College of Business and Management Sciences (CoBAMS–REC) – 3
- Makerere University College of Agricultural and Environmental Sciences (CAES–REC) – 13
- Makerere University College of Veterinary Medicine, Animal Resources and Biosecurity (CoVAB–REC) – 4
Research
Uganda Strengthens Research Ethics Oversight as Makerere and UNCST Equip Ethics Committees for Emerging Scientific Challenges

By Moses Lutaaya
Kampala, Uganda — July 22, 2026
Uganda’s research sector is preparing for a new era of scientific advancement as emerging fields such as artificial intelligence, genomics, digital health; big data analytics and international research collaborations continue to transform the landscape of scientific inquiry. However, experts have emphasized that these developments must be matched with stronger ethical oversight mechanisms to protect research participants, maintain scientific credibility and preserve public trust.
The call was made during the three-day Good Research Regulatory Practice (GRRP) Course for members of Research Ethics Committees (RECs) from Makerere University and other institutions. The training was organized by the Directorate of Research, Innovations and Partnerships at Makerere University in partnership with the Uganda National Council for Science and Technology (UNCST) to strengthen research governance and enhance ethical review practices.
Speaking at the official opening of the course, Prof. Robert Wamala, Makerere University’s Director of Research, Innovation and Partnerships, said ethical oversight remains central to achieving quality research that contributes to national development.
Prof. Wamala said Makerere University remains committed to producing research that addresses Uganda’s priorities while contributing to regional and global scientific advancement. However, he cautioned that research excellence cannot exist without strong ethical safeguards.
“Every research project involving human participants carries with it a profound responsibility to uphold the dignity, rights, safety and well-being of those who make research possible,” Prof. Wamala said.

He described Research Ethics Committees as critical pillars of Makerere’s research ecosystem, emphasizing that their role extends beyond regulatory compliance to protecting scientific credibility and maintaining public confidence.
“The quality, consistency, independence and timeliness of ethical review directly influence the quality of research produced by our institution and the confidence that participants, funders, collaborators and society place in our work,” he said.
Prof. Wamala observed that emerging fields such as artificial intelligence, genomics, digital health, big data analytics and cross-border research collaborations have introduced new ethical questions requiring continuous learning and adaptation.
He said modern ethical oversight demands more than simply following regulations. “It requires critical thinking, sound judgment, an appreciation of emerging technologies and strict adherence to internationally accepted standards of ethical review,” he said.
He noted that the GRRP Course provides an opportunity to harmonize ethical review approaches across Makerere’s Research Ethics Committees, improve institutional capacity and ensure that research involving human participants meets national and international standards.
Prof. Wamala also commended UNCST for its continued partnership with Makerere University in strengthening research governance, describing the collaboration as a reflection of a shared commitment to fostering a research environment that is ethical, responsible, innovative and internationally competitive.
Relatedly, Dr. Hellen Opolot, the Assistant Executive Secretary and Head of the Directorate of Research Management and Quality Assurance at UNCST, called on Research Ethics Committees to continuously strengthen their capacity as Uganda’s research environment becomes increasingly complex.
Dr. Opolot said scientific progress presents immense opportunities but also introduces new ethical, legal and regulatory challenges that require regulators and ethics committees to remain ahead of emerging trends.
She noted that research in Uganda is rapidly expanding, driven by developments in artificial intelligence, genomics, digital health, social and behavioral sciences and multinational collaborative studies.
“As REC members, your role extends beyond reviewing research protocols. You are responsible for safeguarding the rights, dignity and welfare of research participants,” Dr. Opolot emphasized.

She commended the organizers, particularly Professor Wamala for their continued commitment to strengthening research governance through capacity-building initiatives targeting Research Ethics Committees, students and researchers.
“I want to express my sincere appreciation to Professor Wamala for continuously inviting me to these meetings and for organizing important capacity-building programmes, not only for Research Ethics Committees but also for students,” she said.
Dr. Opolot encouraged participants to actively engage in the training, share experiences and develop practical approaches to addressing ethical challenges, noting that many issues facing researchers and regulators require collaboration and informed judgment.
She expressed confidence that the knowledge gained from the training would improve ethical review processes, strengthen post-approval monitoring and promote a culture of research integrity across Uganda.
Prof. Fredrick Nelson Nakwagala, the Chairperson of the Accreditation Committee for Research Ethics in Uganda at UNCST, said the training was aimed at equipping Research Ethics Committees with the skills required to protect human participants and improve research quality.
“The main function of this meeting is to build the capacity of Research Ethics Committees at Makerere University to perform their responsibility of protecting human subjects in research,” Prof. Nakwagala said.
He explained that continuous training remains necessary because ethical standards evolve alongside changes in science and technology.
“Ethics keeps changing because circumstances change. We now have artificial intelligence, mathematical modelling and complex study designs that were not known before. There are also new international and national guidelines on how to protect human participants who volunteer in research,” he said.
Prof. Nakwagala emphasized that Research Ethics Committees play a broader role than approving research proposals. He said they also monitor approved studies to ensure compliance with regulations, scientific standards and legal requirements.
“They monitor approved studies to ensure they are conducted within applicable regulations, scientific standards and the law. This improves both the quality of research proposals and the quality of research implementation,” he said.
He warned that unethical research practices such as plagiarism, fabrication of participants and falsification of data could undermine national development efforts, especially when research findings influence public policy.

“You don’t want research products from scientists who are fraudulent, who fabricate participants or falsify data,” he said. “Research Ethics Committees ensure research is what it claims to be and that the process gives confidence in the results.”
Prof. Nakwagala added that ethics committees play an important role in mentoring postgraduate students by providing a framework that enables them to conduct credible and scientifically sound research.
He linked strong research ethics to Uganda’s development ambitions under the National Development Plan IV, noting that science, technology and innovation are increasingly important in sectors such as agriculture, health, infrastructure, housing and environmental sustainability.
“Ethical oversight is critical in balancing the risks and benefits of development initiatives,” he said.
Addressing concerns about delays in postgraduate research approvals, Prof. Nakwagala said new review timelines introduced by UNCST are expected to improve efficiency while maintaining quality.
“We believe that within a week, most student protocols should receive approval. Only larger studies such as clinical trials require more rigorous review, but even these should not exceed 60 days,” he said.
Day One of GRRP Course Brings Together Experts and Research Ethics Practitioners
Day one of the Good Research Regulatory Practice Course was facilitated by Ms. Irene Semakula Suryani, Dr. Fredrick Nelson Nakwagala, Dr. Robert Sekubugu, Prof. Noah Kiwanuka and Ms. Gladys Nakalema, who guided participants through key areas of ethical review, research governance, regulatory standards and best practices for strengthening Research Ethics Committees.
The training attracted members from various academic units and institutions, including 16 participants from the College of Health Sciences, 5 from the School of Social Sciences, 15 from the College of Agricultural and Environmental Sciences (CAES), 23 from the School of Public Health, 23 from the School of Medicine, 19 from the School of Biomedical Sciences and 5 from the College of Veterinary Medicine and Animal Resources (COVAB).
Research Ethics Committee Leaders Attend Capacity-Building Training
The course also brought together chairpersons of Research Ethics Committees from different schools and colleges who participated in strengthening ethical review systems at Makerere University and beyond. Among those in attendance were chairpersons of the different RECs including Prof. Stella Neema from the School of Social Sciences, Dr. Paul Kutyabami from the College of Health Sciences, and Dr. Joseph Kagagi from the School of Public Health, among other REC leaders.
The participation of REC chairpersons underscored the importance of institutional leadership in promoting responsible research practices, improving review efficiency and ensuring that scientific advancement is guided by integrity, accountability and respect for human dignity.
The GRRP training, running from July 22 to 24, 2026, is part of ongoing efforts by Makerere University and UNCST to strengthen Uganda’s research governance system and ensure that scientific progress is built on ethical foundations.
-

 General1 week ago
General1 week agoUndergraduate Admission Lists 2026/2027
-
 General5 days ago
General5 days agoFreshers’ Joining Instructions 2026/2027
-
 General6 days ago
General6 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General7 days ago
General7 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General6 days ago
General6 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training