Health
Mak Researchers Design National Drowning Prevention Strategy

By Joseph Odoi
Makerere University researchers under Trauma, Injuries and Disability (TRIAD) Unit) have designed a national drowning prevention strategy. This strategy comes at a time when there is sky rocketing cases of drowning in Africa.
Globally, drowning is the third leading cause of unintentional injury death; accounting for 7% of all injuries. Over 90% of the estimated 322,000 annual global drowning deaths occur in low-and middle-income countries.
Although the burden of drowning is believed to be highest in the WHO-African region, data collection and surveillance for drowning in African countries is limited.
In bid to contribute to data driven interventions, Makerere University researchers carried out a study aimed at establishing the availability of drowning data in district-level sources and understanding the reporting of and record keeping on drowning in Uganda.
As part of the study titled: Drowning in Uganda; examining data from administrative sources, researchers engaged various health stakeholders who shared their experiences about drowning and how it can be prevented in communities.
It is upon that background that scholars designed a contextual appropriate strategy for drowning prevention in Uganda under the project titled; Drowning in Uganda; examining data from administrative sources.
According to the researchers, this drowning strategy is first ever in Uganda. ‘’it will be a national document that will guide all the efforts on drowning prevention in the country; and will avoid non-coordinated activities aimed at prevention of drowning. the strategy will also provide for monitoring and evaluation of all activities and interventions for drowning prevention in the country since there will be a government lead agency tasked with this responsibility’ ’explained Mr. Fredrick Oporia who is part of the study team
STRATEGIES TO PREVENT DROWNING
In this study published on semantics scholar among other journals, the researchers came up with the following strategies to counter drowning;
• Setting and enforcing safe boating regulations. • Providing incentives that encourage adherence to boating regulations related to not overloading transport boats and increasing enforcement of boating regulations. • Ensuring boats are fit for purpose and increasing regular inspection of the seaworthiness of boats. • Improving detection and dissemination of information about the weather. • Supporting increased availability and use of lifejackets through subsidy, lifejacket loaner programs, and free lifejacket distribution programs. • Increasing sensitization about safe boating practices, the importance of wearing lifejackets, and limiting alcohol and illicit drug use when boating. Community members, especially children, are vulnerable to drowning in unsafe water sources such as ditches, latrines, wells, and dams. Potential interventions could include: • Modifying access to wells and dams to prevent children or adults from falling in. • Installing boreholes and pumps to enable community members to draw water safely.
Providing safe rescue and resuscitation training to community members and conducting refresher trainings. • Developing and providing low-cost rescue equipment such as boat fenders (rubber and ropes tied to boat on all sides that can assist in the immediate rescue of individuals) and buoyant throwing aids.
To enable ongoing design, implementation, and evaluation of drowning prevention efforts, the researchers note that it is essential to collect data on drowning incidents. Reporting of and record keeping on drowning in Uganda should also be improve according to the researchers namely; Tessa Clemens, Frederick Oporia, Erin M Parker, Merissa, A Yellman, Michael F Ballesteros and Olive Kobusingye
Other Potential interventions highlighted by the researchers include: • Providing records officers with proper training, equipment, and appropriate storage facilities. • Sensitizing the public on the importance of reporting all drowning cases to authorities.
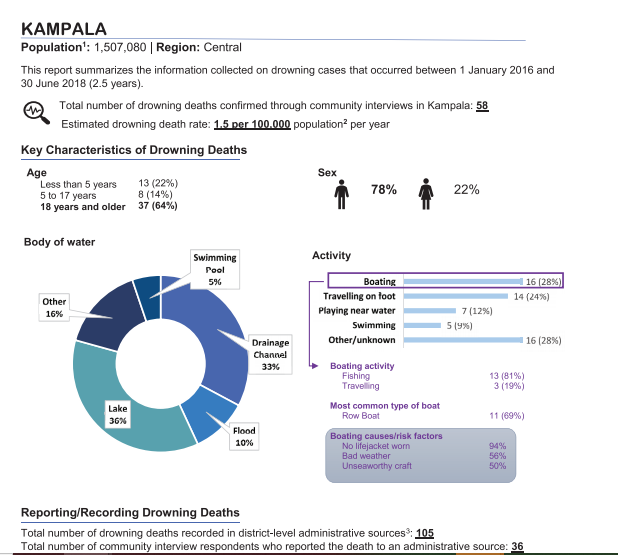
As part of their study findings, the researchers noted that; A total of 1435 fatal and non-fatal drowning cases were recorded; 1009 (70%) in lakeside districts and 426 (30%) in non-lakeside districts.
Of 1292 fatal cases, 1041 (81%) were identified in only one source. After deduplication, 1283 (89% of recorded cases; 1160 fatal, 123 non-fatal) unique drowning cases remained. Data completeness varied by source and variable.
On demographics, fatal victims were predominantly male (85%), and the average age was 24 years. In lakeside districts, 81% of fatal cases with a known activity at the time of drowning involved boating.
What were people doing when they drowned?
Activity at the time of drowning in lakeside districts and non-lakeside districts
• Overall, boating was by far the most common activity that people were engaged in at the time of the drowning incident.
• Other common activities were collecting water/watering cattle and travelling on foot.
• The most common activities that people engaged in prior to drowning were similar in lakeside and non-lakeside districts. However, in non-lakeside districts, more drowning deaths occurred as a result of collecting water or watering cattle than as a result of boating in those districts.
• Almost half (48%) of all drownings occurred while the person was engaged in an occupational activity.
Of the 1,063 people who died from boating-related drowning or suffered a severe boating related drowning incident but survived, 1,007 (95%) were not wearing a lifejacket at the time of the incident.
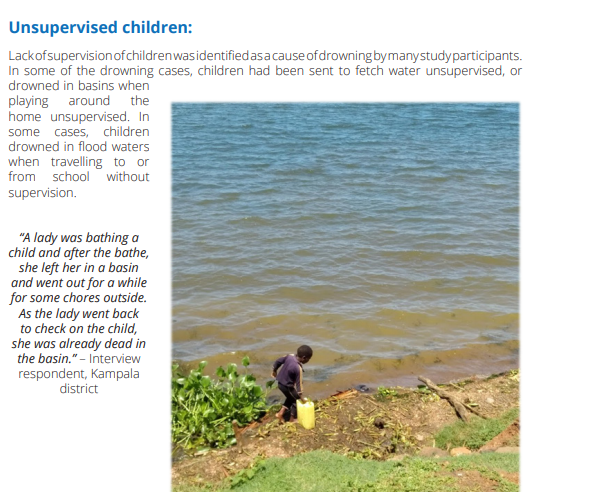
Bathing in water bodies: Study participants indicated that drowning sometimes occurs when people are bathing in lakes, ponds, swamps, and valley dams. People can unexpectedly slip into deep water from shallower areas or rocks.
Crossing flooded rivers and streams:
Attempting to cross flooded rivers and streams during the rainy season was another cause of drowning identified by study participants.
“Currently, people cross from makeshift bridges such as that of round poles. When the river overflows, it covers them. So, you can’t see them; so, you just start guessing: ‘the pole might be here or there’ and in case your guess is wrong, you automatically drown and you will be gone.” an Interview respondent in Kabale district explained
Delayed rescue attempts: Study participants identified the importance of timely rescue and resuscitation to prevent death from drowning. However, they also indicated that community members lack knowledge on how to rescue someone who is drowning.
Alcohol use: Several participants identified alcohol use as a key risk factor for drowning. Participants stated that alcohol use is common, especially in fishing communities. “We have a problem with alcoholism. Many of our colleagues go to the waters when their minds are a bit twisted by the alcohol and on some occasions, this has caused accidents and some of them have drowned just like that.” – Interview respondent, Nakasongola district.
When asked on strategies of preventing drowning, participants suggested the following strategies for preventing drowning:
• Provide affordable and high-quality lifejackets to all water transport users and fishing communities. • Increase sensitization of fishermen and all water transport users on the importance of using lifejackets and avoiding alcohol while boating. • Provide subsidies for large and motorized boats that can be used for safe water travel and fishing to replace small and low-quality boats that are currently in use.
Inspect boats regularly to ensure they are in good travelling condition. • Recruit and deploy more marine police units on all major water bodies to enhance security and quick response to drowning incidents. • Install boat fenders (rubber and ropes tied to boat on all sides) to assist with the immediate rescue of individuals who are involved in a drowning incident. • Provide frequent and safe ferry services to enable water travellers access to safe transportation across rivers and lakes. • Avoid fishing during the moonlight periods to minimize hippopotamus attacks which are more frequent at that time.
“I think these fishermen really need lifejackets for their work and also need to be sensitized on how to manage the engine of the boats that they use for their work. In most cases, these men just learn how to use these boats without having been trained first.” – Interview respondent, Rakai district. Swimming and basic rescue skills said
Moving forward, the researchers recommend that since; drowning is a multisectoral issue, and all stakeholders (local and national government, water transport, water sport, education, fishing, health, and law enforcement) should coordinate to develop a national water safety strategy and action plan.
MORE ABOUT THE STUDY
The study was conducted in 60 districts of Uganda for a period of 2.5 years (from January 1st, 2016 to June 30th, 2018). In the first phase, records concerning 1,435 drowning cases were found in the 60 study districts.
In the second phase, a total of 2,066 drowning cases were identified in 14 districts by community health workers and confirmed through individual interviews with witnesses/family members/friends and survivors of drowning. This work was funded by Bloomberg Philanthropies through the CDC Foundation











As the funding to the higher education sector keeps on reducing due to competing priorities, universities are implored to come up with structures and strategies to attract and win research grants.
Key findings indicate that universities with institutionalized grant management offices, strong and coordinated research teams are better positioned to effectively compete for grants.
Makerere University, in partnership with Northwestern University, is spearheading the E-SMAC G11 Grants Administration and Management workshop from 14th to 17th July 2025, aimed at strengthening grant management offices and systems among the participating universities and entities.
It is envisioned that through this capacity building approach, the workshop which brings onboard over 130 participants from different universities and entities, will address the knowledge and skills gaps among faculty, grant managers, administrators and support staff.
The participating universities and entities include: Makerere University, Uganda Christian University-Mukono, Soroti University, Gulu University, Clarke International University, King Ceasor University, Kyambogo University, Muni University, Mother Kevin University, Uganda Martyrs’ University-Nkozi, Ernest Cook University, Mbarara University of Science and Technology, University of Kisubi, Kabale University, Busitema University, BRAC University, Infectious Diseases Institute, Ministry of Health, and among others.
Makerere University and Northwestern University have built a strong partnership over the past decade through academic exchange, collaborative research, and capacity building initiatives. “Since 2020, the institutions have deepened their collaboration in research administration through the UASP fellowship, sharing best practices and co-developing of sustainable systems to strengthen research management,” said Prof. Sylvia Antonia Nakimera Nannyonga-Tamusuza, Head of Grants Administration and Management Support Unit (GAMSU) at Makerere University.
She informed the participants that Northwestern University has been instrumental in building the capacity of staff at Makerere University in grants writing, management and administration.

Prof. Nannyonga-Tamusuza testified that when she was appointed to head GAMSU, she received comprehensive training from Northwestern University, which enhanced her competences and expertise in the field. She acknowledged Kate Klein from Northwestern University for the mentorship that empowered her with valuable knowledge and skills. She reported that five (5) members of staff from Makerere University had been trained by Northwestern University in grants and research management.
Filled with joy, she introduced the team of experts from Northwestern University namely Kate Klein, Bethany Ekesa and Elizabeth Christian to Makerere University, and applauded them for accepting to be facilitators. Prof. Nannyonga-Tamusuza assured the workshop participants that the team from Northwestern University would not only train them, but would share best practices in grants management and administration as well as networking opportunities.
The training workshop is part of the Expanded Strengthening of Makerere University’s Research Administration Capacity (E-SMAC) program, which focuses on enhancing research administrative systems and staff capacity at Makerere University and its partner institutions. Mordecai Tayebwa is the Program Director and Principal Investigator of the E-SMAC program being implemented from July 2024 to December 2025. The program is funded by the National Institute of Allergy and Infectious Diseases (NIAID).
The workshop provides a platform to build faculty, grant managers and administrators capacity in grant writing and management, foster cross-functional collaboration across departments, strengthen understanding of budget creation, biosketch and funder systems, encourage mentorship and peer to peer learning, and lay a foundation for regular support.
The training tackles four broader themes namely Grants Introduction and Systems, Proposal Development, Capacity Building, and Outcomes and Forward Planning. It covers vital areas such as grant writing, budgeting, funder systems, compliance, and overall grant administration. It features practical sessions, mentorship opportunities, and collaborative learning, with the goal of strengthening pre-award and post-award grant management and improving research productivity and compliance.

Opening the workshop, the Acting Deputy Vice Chancellor (Finance and Administration) at Makerere University, Prof. Winston Tumps Ireeta urged universities to institutionalize grant management offices and policies as well as strengthening research systems through collaborations.
Sharing his experience, Prof. Ireeta informed the participants that he was involved in the strategic discussion that led to the establishment of GAMSU at Makerere University. “We observed that Makerere University School of Public Health had established a grants office, which was instrumental in attracting and winning funds for research. We were inspired by this best practice. Thus, a comprehensive policy was developed to streamline and strengthen grants management across all colleges at the University,” he said.
Prof. Ireeta noted that Makerere University commits to being a research-driven institution, a strategic direction, that needs a strong funding base. ‘Research grants are therefore a key resource,” he said.
Stressing the importance of adhering to the technical details in the grants management processes, Prof. Ireeta appealed to the participants to be active listeners and maximally utilize the moment to learn from the experienced facilitators.

In the same vein, Prof. Nannyonga-Tamusuza, applauded the University Council and Management for the strategic direction undertaken to elevate GAMSU from a Unit to a Directorate. This points to the central role of the grants office in the life cycle of Makerere University. She pointed out that GAMSU reports to the Vice Chancellor through the Deputy Vice Chancellor (Finance and Administration).
Established by the University Council in 2020, GAMSU is a central office at Makerere University. It provides professional and coordinated services across the entire grant life-cycle-from identifying funding and developing proposals to ensuring compliance, project execution, financial oversight, and institutional capacity building. GAMSU works closely with academic and administrative staff to support competitive, well-managed and accountable research.
Focusing on the training workshop, Prof. Nannyonga-Tamusuza called upon the participants to utilize the golden opportunity to deepen their understanding of grants management in advancing research. She acknowledged the role of this collaboration in fostering mutual learning and the sharing of best practices, noting that such initiatives were key in ensuring that research conducted by universities aligns with global standards. She encouraged participants to engage fully in the workshop, collaborate with their peers, and build lasting connections to foster continuous learning.
The Administrative Director of the Havey Institute for Global Health at Northwestern University, Kate Klein, noted that grants administration goes beyond securing funding. She explained that grant administration is about building strong, sustainable systems that support researchers, facilitate collaboration, and ultimately contribute to solving global challenges.
Klein stated that grants administration and management require continuous learning, adaptability, and a strong foundation in regulatory and financial oversight.
“Collaborating and learning from one another is essential,” Klein stated. “When grants administration is effectively managed, it becomes a powerful catalyst for driving impactful change in research, ultimately advancing global initiatives that address the world’s most pressing challenges.”

She urged participants to critically analyze their current systems and identify areas where improvements could be made. By doing so, they would be better positioned to manage grants effectively and maximize their impact. She guided that a research grants administrator should be able to design monitoring frameworks, liaising with funders to address grant-specific issues, coordinating compliance, budgeting and reporting to ensure timely and effective implementation.
Presenting the Existing Support Systems and Principal Investigator (PI) agreements, Prof. Nannyonga-Tamusuza pointed out the critical role of GAMSU in maximizing Makerere University’s access to grants. This is particularly important in the context of limited financial resources, where GAMSU ensures that the university effectively leverages available funding opportunities.
Prof. Nannyonga-Tamusuza explained that GAMSU ensures research projects align with the priorities of funders and comply with both institutional and external regulations. She emphasized that this alignment is essential for securing and managing grants successfully. She stated that oversight offered by GAMSU, helps streamline the process for researchers. She pointed out that grant management is a collaborative process, involving multiple stakeholders across the university, which ensures that the necessary expertise and support are in place to manage grants effectively.
Underscoring the importance of grant negotiations, particularly with sub-award grants, Prof. Nannyonga-Tamusuza clarified that such negotiations are most successful when managed at the institutional level, where GAMSU oversees the entire lifecycle of a grant-from identifying funding opportunities to post-award activities.
Harriet Nambooze, the Project Coordinator at Makerere University School of Health Sciences, provided participants with a detailed guide on navigating the National Institutes of Health (NIH) grant application process. She introduced essential tools such as Grants.gov, eRA Commons, SAM.gov and the NATO Commercial and Government Entity (NCAGE), which are critical for applying and receiving an NIH award.

Nambooze stressed the importance of accurately setting up roles in the eRA Commons system, including Signing Official (SO), Principal Investigator (PI), Account Administrator (AA), and Administrative Official (AO), as well as ensuring that profiles are up-to-date across various systems.
She highlighted the necessity of adhering to NIH’s strict submission deadlines and maintaining active individual and institutional profiles to facilitate timely applications. She recommended that institutions should appoint multiple Signing Officials (SOs), to avoid any delays with the required submissions.
Presenting to the participants, Mordecai Tayebwa shared a detailed, step-by-step guide to starting a new grant application. He explained the key elements of the grant process, including the necessity of including a budget, adhering to specific formatting guidelines, and uploading required documents, such as the foreign justification for international projects.

He pointed out the need of thoroughly verifying the application before submission to ascertain that all required documents are included. “This step is crucial to avoid errors that could delay or jeopardize the submission,” he said.
The first day of the workshop set a strong foundation for enhancing grant administration capacity among the participating universities. Participants were equipped with knowledge and skills in grant systems at the national and global levels.
Day two, will focus on topics such as reading funding opportunity announcements, tailoring writing, budget development and justification, sub-contract management, sub-recipient monitoring, and Memoranda of Understanding (MoUs).
On Day three, the participants will gain a deeper understanding of the Grants Office, financial management, internal controls and reporting, peer review process overview and project closeout.
On Day four, the participants will witness the launch of the MakGAP (Makerere University Grants Professional Initiative), listen to a keynote speech on grants management from the Vice Chancellor of Makerere University, Prof. Barnabas Nawangwe, as well as presentations on professional growth through MakGAP, CRA Exam, and Global Research Administration Networks, and professional recognition of research managers and administrators in Africa and post evaluation.
The first day of the workshop set a strong foundation for enhancing grant administration capacity among the participating universities. Participants were equipped with knowledge and skills in grant systems at the national and global levels.
Day two, will focus on topics such as reading funding opportunity announcements, tailoring writing, budget development and justification, sub-contract management, sub-recipient monitoring, and Memoranda of Understanding (MoUs).
On Day three, the participants will gain a deeper understanding of the Grants Office, financial management, internal controls and reporting, peer review process overview and project closeout.
On Day four, the participants will witness the launch of the MakGAP (Makerere University Grants Professional Initiative), listen to a keynote speech on grants management from the Vice Chancellor of Makerere University, Prof. Barnabas Nawangwe, as well as presentations on professional growth through MakGAP, CRA Exam, and Global Research Administration Networks, and professional recognition of research managers and administrators in Africa and post evaluation.

Based on research led by Max Bobholz and colleagues from Makerere University in Uganda, Essentia Institute of Rural Health, and the Medical College of Wisconsin in the United States.
Adolescence is meant to be a time of holistic growth and self-discovery, but for many Ugandan teenagers, this period is becoming a season of silent mental health struggles. A new study published in PLOS Global Public Health has uncovered a silent but growing crisis: nearly one in five Ugandan secondary school students in the study areas have signs of an emotional disorder. These conditions included anxiety, depression, post-traumatic stress disorder (PTSD), and adjustment disorders often involving excessive worry, sadness, fear, or mood instability. Also, one in 20 adolescents exhibited behavioral issues ranging from attention-deficit/hyperactivity disorder (ADHD) and oppositional defiant disorder to substance use and other risky behaviors like alcohol use.
The study, led by Max Bobholz, a PhD candidate in Public and Community Health at the Medical College of Wisconsin, surveyed a sample of 1,953 students aged 10 to 18 years enrolled in eight secondary schools in Iganga district in Eastern Uganda and Mukono district in Central Uganda. This was one of the most comprehensive efforts yet to understand the prevalence and drivers of mental health challenges among school-going Ugandan adolescents.
“We are looking at a generation facing a complex blend of stressors, namely, academic, social, and emotional,” says Bobholz. “Our findings show that certain groups are especially vulnerable, and schools need to be equipped to respond.”
This study results, published on June 12, 2025 was funded by the Swedish International Development Cooperation Agency (SIDA), a government agency of the Swedish Ministry for Foreign Affairs, through the Makerere University Postdoctoral Fellowship to one of the investigators, Dr. Catherine Abbo. Other researchers included Julia Dickson-Gomez, Arthur Kiconco, Abdul R. Shour, Simon Kasasa, Laura D. Cassidy, and Ronald Anguzu.
According to the study, girls bear a higher emotional burden. Researchers found that female students had nearly two times higher odds of suffering from emotional disorders such as anxiety or depression than their male peers.
Dr. Catherine Abbo, an Adolescent Psychiatrist and Associate Professor at Makerere University, attributes this to both biological and socio-cultural factors. “Puberty brings hormonal shifts that can heighten emotional sensitivity,” she explains. “But just as importantly, Ugandan girls often face intense pressure to conform to gender roles while also navigating issues like body image, harassment, and future uncertainty.” The researchers are calling for gender-sensitive mental health interventions, particularly in schools, where early support could help mitigate long-term mental health issues.

Higher associations in older teens?
Age also emerged as a key associated factor, with each additional year increasing the odds of behavioral disorders by 20%. “As adolescents grow older, they are more prone to risk-taking, impulsivity, and resistance to authority,” explains Dr. Simon Kasasa, a senior lecturer and biostatistician at Makerere University School of Public Health.

“Combine that with academic pressure and identity-related stress, and it’s no surprise we’re seeing more conduct issues in late adolescence,” Dr. Ronald Anguzu, an Assistant Professor in the Institute for Health and Humanity at the Medical College of Wisconsin, added. This study raises critical questions about whether and how Ugandan secondary schools support older students as they transition toward adulthood.
The unseen influence of family mental health
The study also found that adolescents with a family history of mental illness had twice the odds of exhibiting behavioral problems compared to those without such a history.
“This speaks to the intersection of genetics and environment,” says Bobholz. “Living in a household with people affected by mental illness can mean instability, stigma, and lack of emotional support, all of which weigh heavily on a developing mind.”
The authors recommend that school mental health screening include family mental health history and advocate for greater collaboration between education and health sectors to support at-risk households.

Private schools: High marks, higher stress?
Interestingly, students in private schools had 1.4 times the odds of experiencing emotional disorders compared to those in public schools. Private schools, often seen as academic havens, may inadvertently be cultivating high-pressure environments. “There’s an assumption that better facilities mean better well-being,” says Dr. Abbo. “But intense academic competition, social isolation, and a lack of trained counselors can create emotional pressure cookers.”
Previous research in 47 secondary schools across five districts (Rakai, Kyotera, Masaka, Lwengo, and Kalungu) in southwestern Uganda found that economic and family support helped reduce absenteeism among adolescent girls in secondary schools. However, this support did not significantly improve behavior or reduce grade repetition. The region, which includes districts like Rakai and Masaka, also faces a higher burden of HIV, adding to the challenges young people experience.
Meanwhile, a review of data from 42 primary schools in Luwero District identified school-based mental health interventions such as cognitive behavioral therapy and mindset-building approaches as being particularly effective. Researchers now suggest that integrating these strategies, along with efforts to reduce school violence, could go a long way in improving the mental health of Ugandan adolescents.
A-Level pressure: Academic ambition meets mental health strain
The study also found a correlation between advanced (A’level) education and increased risk of emotional disorders. “We selected one school district from each region based on population and past academic performance. As these students prepare for university or the job market, the pressure to succeed becomes enormous,” says Kasasa. “They’re facing a future full of uncertainty, with very little structured mental health support to help them cope.”

A wake-up call for Uganda’s education and health systems
The authors of this study assert the urgent need for school-based mental health programs, especially in private and A-level institutions. These programs should offer routine screening, emotional support, and training for teachers to recognize warning signs of mental health disorders.
Importantly, this study adds weight to calls for a national adolescent mental health policy, tailored to Uganda’s context, with interventions that bridge health, education, and social services.
“Our data shows that mental health challenges are not a fringe issue,” says Bobholz. “They are widespread, significant, and deeply tied to school, home, and society.”
The COVID-19 school closures between 2020 and 2022 deepened feelings of isolation and financial strain, with out-of-school adolescents reporting depression rates as high as 21.5% to 50% higher than their peers who remained in class, according to research published in February 2025. Yet Uganda invests less than 1% of its health budget in mental health, with just one psychiatrist per million people, leaving many teens to cope through cheap alcohol used by 28% of urban youth or untrained healers, as reported by the government paper The New Vision in April 2025. With only 26% of students completing lower secondary school and 35% of the population under age 24, these mental health challenges now pose a serious threat to the country’s future.
Mercy Akankunda of Proven Foundation, a Ugandan NGO supporting vulnerable groups, warns that mental health struggles are quietly eroding the well-being of the country’s youth, over 12 million strong and making up 35% of the population. “These teens are not just statistics. They are the future of Uganda, she asserts. If Uganda hopes to reap the dividends of its young population, addressing adolescent mental health must become and remain a national priority, not just for treatment, but for prevention, resilience, and hope.
Reference:
Bobholz, M., Dickson-Gomez, J., Abbo, C., Kiconco, A., Shour, A.R., Kasasa, S., Cassidy, L.D., & Anguzu, R. (2025). Correlates of behavioral and emotional disorders among school-going adolescents in Uganda. PLOS Global Public Health. Read the study here

-

 General2 weeks ago
General2 weeks agoRe-advert: Admission to Undergraduate Programmes 2025/2026
-

 General1 week ago
General1 week agoRe-Advert for Applications for Diploma and Certificate Training
-

 General5 days ago
General5 days agoMakerere University Fees Waiver for 40 First Year Female Students 2025/2026
-

 General2 weeks ago
General2 weeks agoPress Statement on Ranking
-

 Health1 week ago
Health1 week agoCall for Applications: Responsible Conduct of Research (RCR) Training Course