Health
Mak Researchers Design National Drowning Prevention Strategy

By Joseph Odoi
Makerere University researchers under Trauma, Injuries and Disability (TRIAD) Unit) have designed a national drowning prevention strategy. This strategy comes at a time when there is sky rocketing cases of drowning in Africa.
Globally, drowning is the third leading cause of unintentional injury death; accounting for 7% of all injuries. Over 90% of the estimated 322,000 annual global drowning deaths occur in low-and middle-income countries.
Although the burden of drowning is believed to be highest in the WHO-African region, data collection and surveillance for drowning in African countries is limited.
In bid to contribute to data driven interventions, Makerere University researchers carried out a study aimed at establishing the availability of drowning data in district-level sources and understanding the reporting of and record keeping on drowning in Uganda.
As part of the study titled: Drowning in Uganda; examining data from administrative sources, researchers engaged various health stakeholders who shared their experiences about drowning and how it can be prevented in communities.
It is upon that background that scholars designed a contextual appropriate strategy for drowning prevention in Uganda under the project titled; Drowning in Uganda; examining data from administrative sources.
According to the researchers, this drowning strategy is first ever in Uganda. ‘’it will be a national document that will guide all the efforts on drowning prevention in the country; and will avoid non-coordinated activities aimed at prevention of drowning. the strategy will also provide for monitoring and evaluation of all activities and interventions for drowning prevention in the country since there will be a government lead agency tasked with this responsibility’ ’explained Mr. Fredrick Oporia who is part of the study team
STRATEGIES TO PREVENT DROWNING
In this study published on semantics scholar among other journals, the researchers came up with the following strategies to counter drowning;
• Setting and enforcing safe boating regulations. • Providing incentives that encourage adherence to boating regulations related to not overloading transport boats and increasing enforcement of boating regulations. • Ensuring boats are fit for purpose and increasing regular inspection of the seaworthiness of boats. • Improving detection and dissemination of information about the weather. • Supporting increased availability and use of lifejackets through subsidy, lifejacket loaner programs, and free lifejacket distribution programs. • Increasing sensitization about safe boating practices, the importance of wearing lifejackets, and limiting alcohol and illicit drug use when boating. Community members, especially children, are vulnerable to drowning in unsafe water sources such as ditches, latrines, wells, and dams. Potential interventions could include: • Modifying access to wells and dams to prevent children or adults from falling in. • Installing boreholes and pumps to enable community members to draw water safely.
Providing safe rescue and resuscitation training to community members and conducting refresher trainings. • Developing and providing low-cost rescue equipment such as boat fenders (rubber and ropes tied to boat on all sides that can assist in the immediate rescue of individuals) and buoyant throwing aids.
To enable ongoing design, implementation, and evaluation of drowning prevention efforts, the researchers note that it is essential to collect data on drowning incidents. Reporting of and record keeping on drowning in Uganda should also be improve according to the researchers namely; Tessa Clemens, Frederick Oporia, Erin M Parker, Merissa, A Yellman, Michael F Ballesteros and Olive Kobusingye
Other Potential interventions highlighted by the researchers include: • Providing records officers with proper training, equipment, and appropriate storage facilities. • Sensitizing the public on the importance of reporting all drowning cases to authorities.
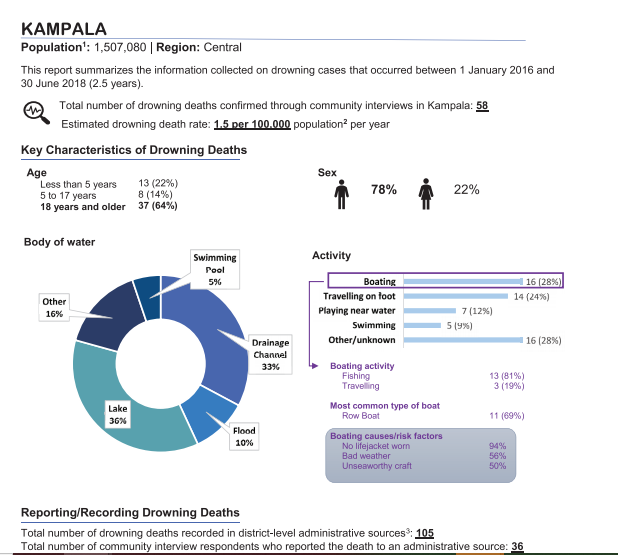
As part of their study findings, the researchers noted that; A total of 1435 fatal and non-fatal drowning cases were recorded; 1009 (70%) in lakeside districts and 426 (30%) in non-lakeside districts.
Of 1292 fatal cases, 1041 (81%) were identified in only one source. After deduplication, 1283 (89% of recorded cases; 1160 fatal, 123 non-fatal) unique drowning cases remained. Data completeness varied by source and variable.
On demographics, fatal victims were predominantly male (85%), and the average age was 24 years. In lakeside districts, 81% of fatal cases with a known activity at the time of drowning involved boating.
What were people doing when they drowned?
Activity at the time of drowning in lakeside districts and non-lakeside districts
• Overall, boating was by far the most common activity that people were engaged in at the time of the drowning incident.
• Other common activities were collecting water/watering cattle and travelling on foot.
• The most common activities that people engaged in prior to drowning were similar in lakeside and non-lakeside districts. However, in non-lakeside districts, more drowning deaths occurred as a result of collecting water or watering cattle than as a result of boating in those districts.
• Almost half (48%) of all drownings occurred while the person was engaged in an occupational activity.
Of the 1,063 people who died from boating-related drowning or suffered a severe boating related drowning incident but survived, 1,007 (95%) were not wearing a lifejacket at the time of the incident.
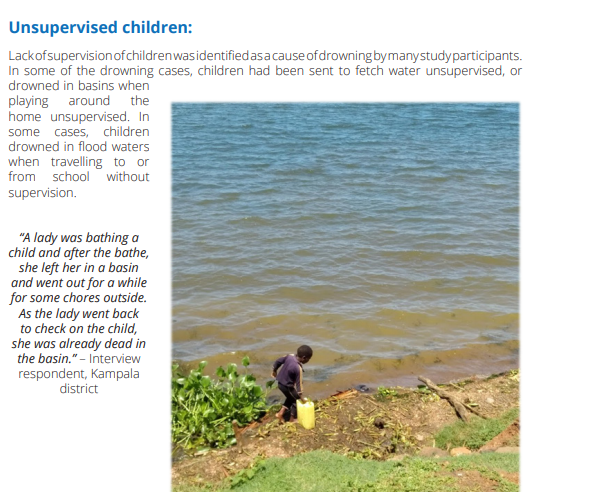
Bathing in water bodies: Study participants indicated that drowning sometimes occurs when people are bathing in lakes, ponds, swamps, and valley dams. People can unexpectedly slip into deep water from shallower areas or rocks.
Crossing flooded rivers and streams:
Attempting to cross flooded rivers and streams during the rainy season was another cause of drowning identified by study participants.
“Currently, people cross from makeshift bridges such as that of round poles. When the river overflows, it covers them. So, you can’t see them; so, you just start guessing: ‘the pole might be here or there’ and in case your guess is wrong, you automatically drown and you will be gone.” an Interview respondent in Kabale district explained
Delayed rescue attempts: Study participants identified the importance of timely rescue and resuscitation to prevent death from drowning. However, they also indicated that community members lack knowledge on how to rescue someone who is drowning.
Alcohol use: Several participants identified alcohol use as a key risk factor for drowning. Participants stated that alcohol use is common, especially in fishing communities. “We have a problem with alcoholism. Many of our colleagues go to the waters when their minds are a bit twisted by the alcohol and on some occasions, this has caused accidents and some of them have drowned just like that.” – Interview respondent, Nakasongola district.
When asked on strategies of preventing drowning, participants suggested the following strategies for preventing drowning:
• Provide affordable and high-quality lifejackets to all water transport users and fishing communities. • Increase sensitization of fishermen and all water transport users on the importance of using lifejackets and avoiding alcohol while boating. • Provide subsidies for large and motorized boats that can be used for safe water travel and fishing to replace small and low-quality boats that are currently in use.
Inspect boats regularly to ensure they are in good travelling condition. • Recruit and deploy more marine police units on all major water bodies to enhance security and quick response to drowning incidents. • Install boat fenders (rubber and ropes tied to boat on all sides) to assist with the immediate rescue of individuals who are involved in a drowning incident. • Provide frequent and safe ferry services to enable water travellers access to safe transportation across rivers and lakes. • Avoid fishing during the moonlight periods to minimize hippopotamus attacks which are more frequent at that time.
“I think these fishermen really need lifejackets for their work and also need to be sensitized on how to manage the engine of the boats that they use for their work. In most cases, these men just learn how to use these boats without having been trained first.” – Interview respondent, Rakai district. Swimming and basic rescue skills said
Moving forward, the researchers recommend that since; drowning is a multisectoral issue, and all stakeholders (local and national government, water transport, water sport, education, fishing, health, and law enforcement) should coordinate to develop a national water safety strategy and action plan.
MORE ABOUT THE STUDY
The study was conducted in 60 districts of Uganda for a period of 2.5 years (from January 1st, 2016 to June 30th, 2018). In the first phase, records concerning 1,435 drowning cases were found in the 60 study districts.
In the second phase, a total of 2,066 drowning cases were identified in 14 districts by community health workers and confirmed through individual interviews with witnesses/family members/friends and survivors of drowning. This work was funded by Bloomberg Philanthropies through the CDC Foundation











Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General11 hours ago
General11 hours agoUndergraduate Admission Lists 2026/2027
-
 General6 days ago
General6 days agoFreshers’ Joining Instructions 2026/2027
-
 General1 week ago
General1 week agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General1 week ago
General1 week agoMakerere University Welcomes 2026/2027 Freshers
-

 General1 week ago
General1 week agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training