Health
Research Links Social Support to Improved Contraceptive Decision-Making for Women

Researchers at Makerere University School of Public Health (MakSPH) are urging the Ugandan government to boost healthcare funding to enhance reproductive health services. Dr. Dinah Amongin, an obstetrics and gynecology expert at MakSPH, has expressed concern about the lack of access to family planning methods, which forces women to use less preferred options due to unavailability.
Dr. Amongin notes that within just six months to a year of using contraception, some women encountered issues and switched methods. This highlights the need for the Ministry of Health to improve the availability of various contraceptive options. A rights-based approach to contraception ensures that women have access to a range of methods, preventing situations where desired options are unavailable at health facilities.
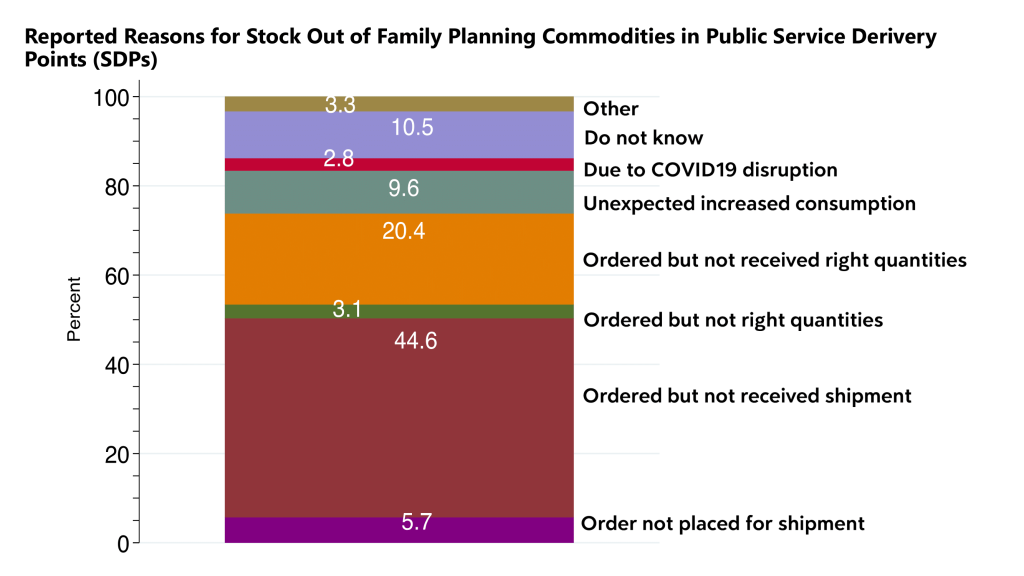
“Stockouts are a significant issue, and this extends to parliamentary discussions on health sector budgets. As we focus on human capital development and improving maternal and newborn health outcomes, we must consider crucial components like preventing unwanted pregnancies through family planning. The budget allocation for the health sector directly impacts this issue. When women cannot access their preferred contraceptive methods due to stockouts, it reflects a failure in our legislative and budgeting processes. This situation forces women to switch to fewer desirable methods, which is not acceptable,” says Dr. Amongin.
Adding that; “These are things we need to continue discussing as a country but we must invest into family planning. We can talk about human capital development but until we step up and actually support women to prevent unwanted pregnancies, support them in their decisions of whether she wants to use a method for contraception or not. That is her choice. We must make sure access to the methods of her choice is actually addressed.”

Dr. Amongin’s comments follow a recent study on the I-CAN/Nsobola/An atwero social support intervention, piloted in Mayuge and Oyam districts in 2023. The study highlights that social support significantly improves women’s ability to make informed contraceptive choices, potentially leading to better reproductive health outcomes.
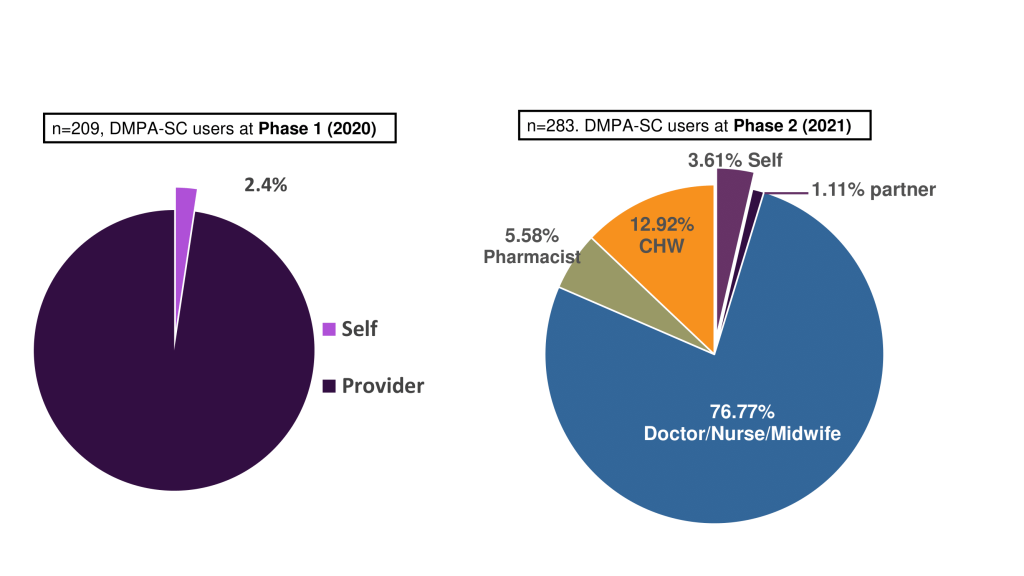
Part of the Innovations for Choice and Autonomy (ICAN) project, the study shows that self-injection with DMPA-SC (Sayana Press) could increase contraceptive use, especially among women with limited access to healthcare. Despite the rollout of this method in 2017, its use remains low in Uganda. Sayana Press as popularly known is a subcutaneous depot medroxyprogesterone acetate (DMPA-SC). It is a hormonal birth control shot, administered under the skin and is an all-in-one contraceptive that puts women in charge of their reproductive health.
Social support boosts self-efficacy, enhances privacy, and reduces access barriers, making self-management easier. Family planning helps manage the number and timing of children, lowering maternal and infant mortality rates and reducing complications from pregnancy. Conversely, unmet contraceptive needs can lead to unintended pregnancies and their associated risks.

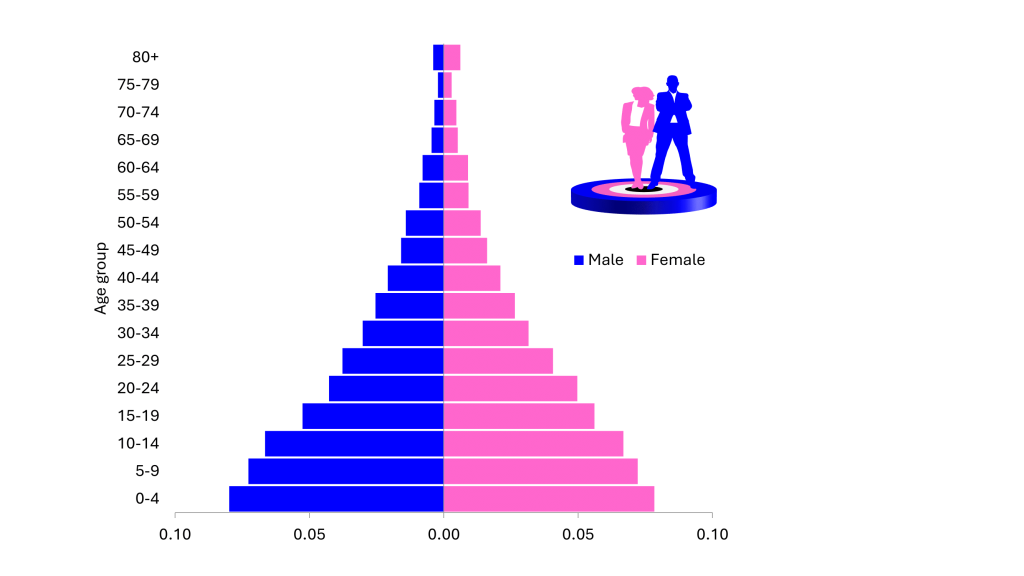
In Uganda, 52% of pregnancies are unwanted or mistimed, with over 43% due to unmet family planning needs. The country’s youthful population complicates the issue, with 50% under 17 years old, at least according to the recent National Population Census. Notably, 10% of girls, one in every 10 girls you encounter, has already had sex before she turns 15 years, and 20% of boys, two in 10 boys have engaged in sexual intercourse by the same age.
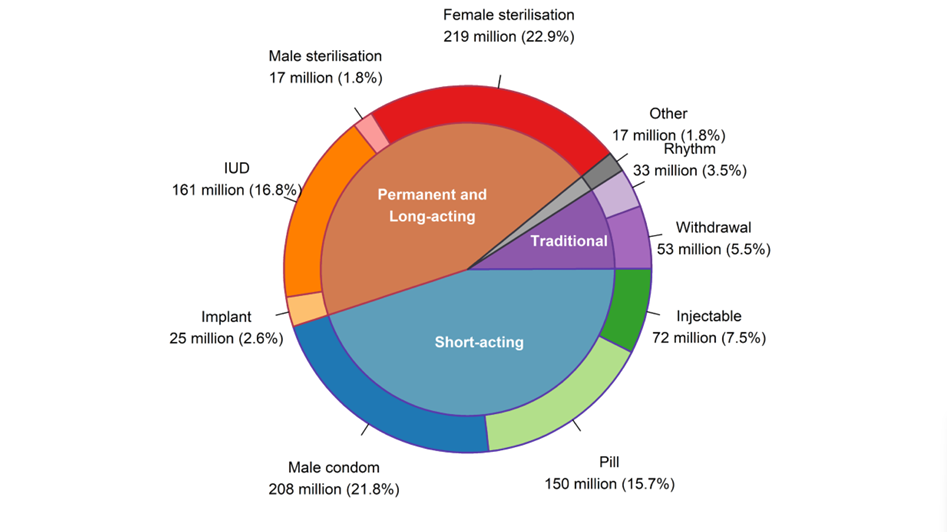
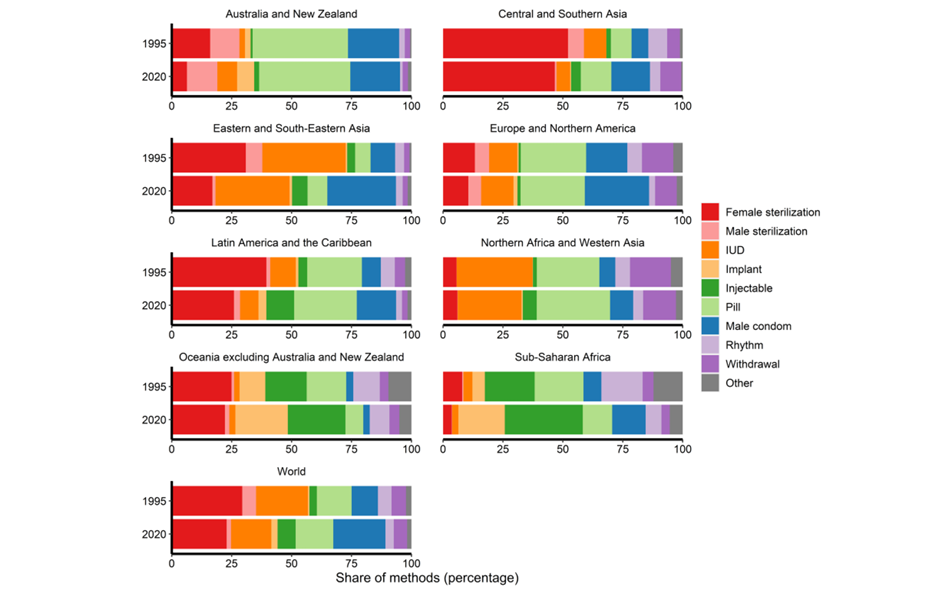
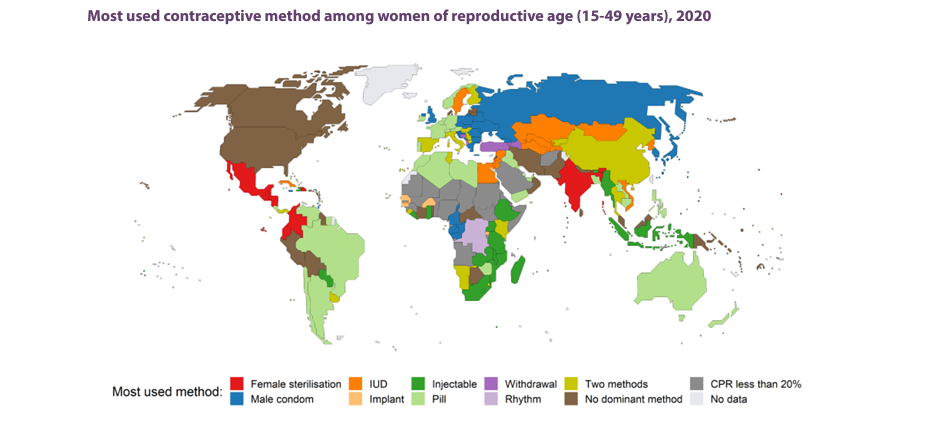
Methods of contraception include oral contraceptive pills, implants, injectables, patches, vaginal rings, intra uterine devices, condoms, male and female sterilization, lactational amenorrhea methods, withdrawal and fertility awareness-based methods.
Global statistics show that 77.5% of women aged 15–49 had their family planning needs met with modern methods in 2022, up from 67% in 1990. In sub-Saharan Africa, the proportion of women who have their need for family planning satisfied with modern methods (SDG indicator 3.7.1) continues to be among the lowest in the world at 56 per cent. Nevertheless, it also increased faster than in any other region of the world, having more than doubled since 1990, when this proportion was only 24 per cent.
Among 1.9 billion women of reproductive age (15-49 years), an estimated 874 million women use a modern contraceptive method and 92 million, a traditional contraceptive method. The number of modern contraceptive users has nearly doubled worldwide since 1990 (from 467 million). Yet, there are still 164 million women who want to delay or avoid pregnancy and are not using any contraceptive method, and thus are considered to have an unmet need for family planning.
Slow progress is due to factors like limited method choices, restricted access, fear of side effects, cultural opposition, and gender-based barriers.
Between 2015 and 2019, there were 121 million unintended pregnancies annually worldwide – 48 per cent of all pregnancies. Despite decreases in the rate of unintended pregnancy in all regions over the past three decades, nearly one in 10 women in sub-Saharan Africa, Western Asia and Northern Africa, and Oceania (excluding Australia and New Zealand) continue to experience an unintended pregnancy every year

In Uganda, where healthcare services are stretched thin and women juggle numerous responsibilities, accessing contraceptives can be challenging.
Dr. Amongin emphasizes that self-injection methods like DMPA-SC, also known as Sayana Press could ease the burden on women facing long queues and logistical challenges at health facilities. “This method allows for discretion and reduces the need for frequent visits, which is crucial for women with busy lives,” she says.
Researchers argue that the health sector’s budget should include substantial funding for family planning. The high cost of inaction is evident: neglecting family planning leads to unplanned pregnancies, which ultimately burdens families and the nation. Addressing this issue early in the life cycle is crucial to prevent these long-term consequences.
“This is the gist of the matter behind all our research, that a woman’s preference needs to be respected. The health facilities must stock commodities so that when a woman is in need, she actually gets it,” noted Dr. Amongin.
Dr. Peter Waiswa, an Associate Professor at MakSPH, stresses the importance of informed choice in family planning. ICAN studies across Kenya, Malawi, Nigeria, and Uganda show that self-injection benefits all women, including young adolescents. “Supporting young people to make informed choices helps prevent unintended pregnancies,” says Prof. Waiswa.
“We spent four years trying to understand which women benefit from injecting themselves. And we found that all women benefit from it, including younger children. Because younger children in Uganda, whether we hide our heads in the sand or not, especially those 12 years and above are having sex and some of them using contraceptives,” Professor Waiswa says.

What is factually true is that by age 18, 60% of Ugandans have reported having sexual intercourse. Despite the benefits, dropout rates from family planning methods remain high due to side effects and lack of support. Dr. Waiswa also, a Public Health specialist, critique and dreamer for better health systems for mothers, newborns and children in Africa calls for better education and support to address these issues.
“As a way of being supported in a safe space whereby people are not asking questions, they are not fearing parents, they are not fearing other people, then they can use the methods. What we did in Mayuge and Oyam, we trained women who are users of family planning. To identify people who need to use family planning but are not currently using and then they go and see whether they can use or not. And we found that when people are supported, those groups which are currently not being reached can be reached by family planning,” argues Prof. Waiswa.
A 2021 study found that contraceptive discontinuation significantly impacts the effectiveness of family planning services, leading to higher fertility rates, unwanted pregnancies, and induced abortions.
Analysis of data from PMA 2020 show that 6.8% of women discontinued contraceptive use, with discontinuation linked to factors such as age, marital status, method type, and health concerns. The study suggests prioritizing interventions to encourage contraceptive use among young people and promoting partner involvement and awareness, as many contraceptive methods are not discreet.
Prof. Waiswa is concerned of the high dropout rate from family planning methods, where many women discontinue use due to side effects, a need for better education and support.
“We need to see how to educate women so that they are informed when they are choosing a method to use. They need to have enough information because when they discontinue, the method can be ineffective, can cause side effects, but also these methods are expensive, so they waste money. There are a lot of those who change to other methods. We are learning a lot on the use of family planning why we still have a large unmet need,” says Prof. Waiswa.
Ms. Roseline Achola, Technical Specialist for Sexual and Reproductive Health and Self-Care at the Ministry of Health, hailed the MakSPH study on self-injection contraception. She noted that the findings will help her enhance support for self-care initiatives. However, she expressed that only 29% of women willing to self-inject as indicated in the study is still low, highlighting a need to address barriers to increase acceptance as well as managing sexually active adolecents. “We must discuss how to handle minors seeking contraception to prevent unintended pregnancies,” she says.
On Friday August 23, 2024, the Daily Monitor reported, an increase in young girls adopting family planning to combat teenage pregnancies and school dropouts. Quoting data from the Uganda Health Information System, statistics show that between March 2023 and March 2024, 2,476 girls under 15 had their first antenatal care visit, and 1,755 gave birth. The highest number of pregnancies among this age group was in Oyam district.
In this period, Lango subregion saw 52 pregnancies among this age group, with Oyam district recording the highest at 10 cases. The 2021 UNFPA fact sheet indicates that Busoga region, particularly Kamuli and Mayuge districts, has the highest rates of teenage pregnancies, with 6,535 and 6,205 cases respectively.
“As the country, it’s clear that adolescents are limited to access to contraception because of so many reasons. For us as a Ministry, any woman between the age of 15 to 49 is a woman of reproductive age and that tells you that she is capable of getting pregnant and when such a girl of probably 15 years goes to a facility to seek for contraception, it rings a message that actually she is sexually active. So how do we handle her? So that is a matter of discussion for the country.
It is a matter that the nation needs to decide on, because we all know the girls are getting pregnant, the girls want to use contraception, but they have no access because of the fact that they are children,” wondered Achola.

Unintended pregnancies and Uganda’s abortion paradox
Abortion in Uganda, is largely illegal except in specific circumstances. It contributes to maternal death due to unsafe practices. Between 2010 and 2014, WHO reported that 30.6million abortions conducted were safe and 25.1million were unsafe. 97% of these occurred in developing countries. In East Africa, the total number of abortions per year according to the Lancet are around 2.65million.
The Ministry of Health’s HMIS data show a rise in abortion cases, with 96,620 reported between July 2020 and June 2021in both government and private health facilities.
Another recent study on the quality of post-abortion care by MakSPH researchers Assoc. Prof. Lynn Atuyambe, Dr. Justine Bukenya, Dr. Arthur Bagonza and Mr. Sam Etajak highlights the need for accurate post-abortion care data to improve healthcare planning and policymaking.
Dr. Arthur Bagonza, a Public Health Consultant and Research fellow with specialization in health systems at MakSPH and one of the uality of post-abortion care has called for accurate abortion data to improve healthcare planning and policymaking. He notes that health workers often avoid documenting abortion data due to legal fears and calls for reforms to restrictive laws to ensure accurate reporting without legal repercussions.
“All assessed health facilities reviewed in our study achieved a 100% timeliness rate for report submissions. However, significant disparities were observed in data accuracy between different levels of health facilities, with lower-level facilities (HC IIs and HC IIIs) showing higher rates of data discrepancies,” says Dr. Bagonza.

According to Dr. Amongin, the high incidence of early sexual activity among Uganda’s youth is a pressing public health issue.
“We know as a country many women continue to die following unsafe abortions; abortions for pregnancies that they did not want. And these abortions are highest among adolescents and also other women categories.
We would want to ensure that we actually enhance access to contraceptives, but making it easier for them to have it and putting the power in the hands of a woman to as much extent as we can. So that a woman can practice what we call self-care, but of course she also will need the support of the healthcare system. But we want this power in women’s hands because of all the challenges that the women actually can encounter in accessing these methods,” she said.
On her part, Achola insists that abortion should not be a last resort for women and urges them to abstain or use protective means in order to avoid unwanted pregnancies. She notes that as long as abortion remains illegal in Uganda, many health workers will avoid addressing it, leading people to unsafe alternatives.
“I can’t be happy because abortion means we have failed to give people a method of their choice to prevent that pregnancy. Or the people are not able to access contraception to prevent unintended pregnancies. Abortion is not the last resort, it’s not a solution because it has its own complications as well,” says Achola.

Despite this, Achola, notes most of the women who walk in health facilities with post-abortion complications must be attended to. “Whereas we don’t encourage people to do abortions, as Ministry of Health we are mandated to handle all complications for anyone who walks in our facilities because our priority is to save life. We want to urge women to avoid certain things. Why should you wait for unintended pregnancy to occur and then abort?”
Dr. Charles Olaro, a Senior Consultant Surgeon and the Director Health services – Curative in the Ministry of Health highlights the financial burden on individuals seeking health services and suggests exploring private sector opportunities and community-based approaches to improve access. “We need to balance values and rights while addressing access barriers,” he notes.
According to Dr. Olaro, the autonomy and agency of women in sexual and reproductive health, particularly in African cultures remain a challenge where social norms may require women to defer decisions to their partners.

He notes that there is a high burden of abortion and self-harm, with a significant portion of maternal mortality attributed to sepsis, which is often a result of unsafe abortions in Uganda.
“We still need evidence to ensure that access barriers are addressed. And this is a question I keep on asking Makerere University, yes, we have a young population but how are these people accessing contraceptives. Other issue we have to deal with is complex. I know we have to do a balance between values and rights, but we will be able to look at that when they gain the success to do it.”
Dr. Olaro points out that individuals often face a financial burden in health services, spending more on prescriptions than on the medications themselves. He suggests exploring private sector opportunities and a community-based approach to improve access to healthcare.
NB: The PMA surveys are spearheaded by Associate Professor Fredrick Makumbi and Dr. Simon Kibira of MakSPH, with support from the Uganda Bureau of Statistics and the Ministry of Health. The initiative also receives funding from the Bill & Melinda Gates Foundation, The Children’s Investment Fund Foundation (CIFF), and is supported by the Bill & Melinda Gates Institute for Population and Reproductive Health at Johns Hopkins University and Jhpiego.











Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General7 days ago
General7 days agoUndergraduate Admission Lists 2026/2027
-
 General5 days ago
General5 days agoFreshers’ Joining Instructions 2026/2027
-
 General6 days ago
General6 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General7 days ago
General7 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General6 days ago
General6 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training