Health
Harriet Aber’s Research Uncovers Uganda’s Hidden Crisis of Child Substance Use

In Uganda, children arrive at health facilities every day with fever, cough, injuries or routine illnesses. What health workers rarely recognise is that some of these children are already living with alcohol or other substance use disorders, conditions that complicate diagnosis, delay treatment, and quietly undermine children’s health, development, and long-term wellbeing.
This hidden reality was uncovered by Dr. Harriet Aber Odonga during her doctoral research at Makerere University School of Public Health (MakSPH). Her PhD study, titled “Substance Use among Children in Mbale, Uganda: Health System Landscape and Support Structures,” examined how Uganda’s health system detects and responds to substance use among children aged six to 17 years.
The findings revealed a problem far more widespread than many health workers and caregivers assumed. Nearly one in four children attending health facilities showed signs of alcohol or other substance use problems, with alcohol the most common substance. In the study, a child was classified as having a “probable” substance use disorder when responses to a standard screening questionnaire indicated harmful or dependent patterns of use requiring further clinical assessment.

The discovery adds urgency to an already serious public health challenge. Globally, alcohol and other substance use is responsible for one in five deaths and contributes to more than 200 disease and injury conditions, according to WHO. Across Africa, alcohol alone accounts for 6.4 per cent of all deaths and 4.7 per cent of disability-adjusted life years. In Uganda, alcohol use disorder affects roughly 7.1 per cent of the population and contributes to about 7% of all deaths, while research among young people shows that alcohol exposure often begins early in life.
Despite these risks, most policy and research attention has historically focused on adults and older adolescents. Much less is known about children who begin experimenting with alcohol and other substances earlier in their childhood, a gap Aber set out to examine by studying how Uganda’s health system identifies and responds to substance use among children.

A research question begins
Aber’s interest in the subject began unexpectedly. “I remember seeing a notice calling for PhD students to research child alcohol use,” Dr. Aber recounted. “The phrase struck me immediately. I could not believe that children were drinking alcohol. That moment sparked my curiosity, so I began reviewing the literature on the subject in Uganda. During that search, I came across a study documenting alcohol use among children as young as five years old. That finding was deeply unsettling and raised many questions for me.”
With a longstanding interest in child health, Aber saw the research as an opportunity to investigate a problem that had received little systematic attention. What began as disbelief developed into a doctoral investigation examining how Uganda’s health system identifies and responds to substance use among children. She began her doctoral studies in 2021 at MakSPH under the supervision of Dr. Juliet N. Babirye, Prof. Fred Nuwaha, and Prof. Ingunn Marie S. Engebretsen from the University of Bergen, Norway. She defended her thesis on October 25, 2025, before graduating during Makerere University’s 76th graduation ceremony on February 25, 2026.

Investigating the health system response
Aber’s study examined four key questions. It measured how common substance use disorders are among children visiting health facilities. It assessed whether health facilities are equipped to screen and manage these cases. It evaluated whether screening tools are acceptable to children, caregivers, and health workers. It also examined how families seek help when children begin using substances.
To answer these questions, the research used a mixed-methods design combining quantitative surveys and qualitative interviews. Aber collected data from 834 children attending health facilities in Mbale District, assessed 54 health facilities in the district to determine their readiness to screen and manage substance use disorders, and interviewed health workers, caregivers, and children to understand experiences of care and barriers to seeking help. Additional surveys involving 602 children and 355 caregivers examined help-seeking patterns and support structures.
Quantitative data were analysed to estimate prevalence and identify associated risk factors, while qualitative interviews provided insight into how families, communities and health workers respond when children begin using substances.
What the research found

Data collected between 2023 and 2024 across health facilities in Mbale District in Eastern Uganda showed that substance use among children was far more common than many health workers and caregivers assumed. Alcohol use disorder emerged as the most prevalent form of substance use disorder among children in the study. The analysis also showed that children were significantly more likely to use substances if they were exposed to peer or sibling use, lived in lower-income households, or experienced strained relationships with caregivers.
The research also revealed major health system gaps. Only 19 of the 54 health facilities assessed, representing 35 per cent, met the minimum readiness criteria required to screen, diagnose or manage substance use disorders. Many facilities lacked trained staff, standardised screening guidelines, and clear referral pathways for specialised care.
Aber explained that substance use often goes undetected because it is rarely the primary reason children visit health facilities. “Substance use is hidden,” she asserted, reflecting on evidence from her doctoral study. “While health workers are treating other illnesses, some children coming to these facilities are already struggling with alcohol or other substances.”
She added that early substance use can have lasting consequences for children’s development. “Risk was higher among children exposed to peer or sibling substance use, lower household income, lower caregiver education, and strained child-caregiver relationships. The public should be concerned because early substance use affects brain development, mental health, education completion, and long-term well-being.”
Families often navigate the problem alone

Her research also examined how families and communities respond when children begin using substances. She found formal help-seeking to be rare. Many caregivers relied on informal networks, including relatives, teachers, religious leaders, and local authorities. Health services were seldom the first point of support.
Meanwhile, punitive responses such as discipline or punishment were sometimes used by caregivers attempting to stop the behaviour of substance use among children, but these responses rarely addressed the broader social and family pressures influencing the vice.
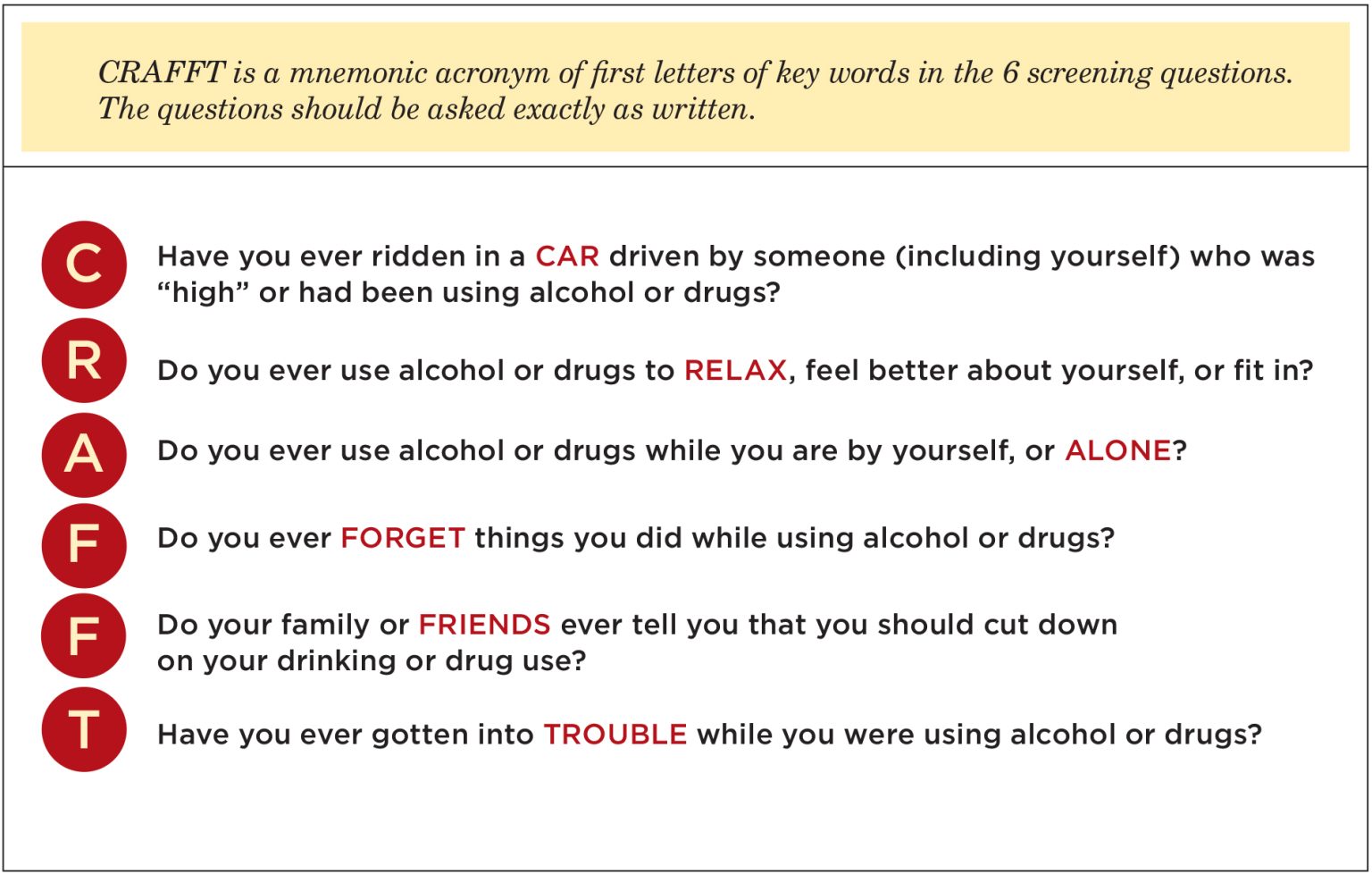
One encouraging finding emerged from her study’s assessment of early detection tools. Aber evaluated the use of the CRAFFT screening tool, a short set of structured questions used by health workers to identify whether a child may be using alcohol or other substances. Children, caregivers, and health workers generally found the questions from the tool easy to understand and acceptable to use. In the study, over 85 per cent of children reported the questions were easy to answer, and nearly nine in ten caregivers were comfortable with the screening process.
These findings, however, suggest that routine early detection could be integrated into primary healthcare within the communities. “If policymakers were to act on one finding from my research, I would prioritise integrating routine, age-appropriate substance use screening into primary healthcare,” Aber argued. “With proper training and referral systems, health workers can identify early risk and support children before the problem escalates.”
Training across nutrition, public health and health systems
Aber’s approach to the problem reflects a research journey shaped by training across multiple areas of child and public health. She first studied Food Science and Technology at Kyambogo University, graduating in 2011, before specialising in Nutrition during her Master of Public Health at Makerere University, graduating in 2015, before embarking on her doctoral training in Public Health at the School, completing in 2025 to graduate at Makerere University 76th Congregation.

Before beginning her PhD, she worked on nutrition research and later coordinated studies examining climate risks, anticipatory humanitarian action and community health systems. This background shaped how she approached substance use among children, not as an isolated behavioural problem but as an issue influenced by broader health and social conditions.
“I do not see child substance use as a problem with a single cause,” she noted. “It is influenced by biological, psychological, social, and system-level factors. My nutrition training helped me appreciate how substance use intersects with broader child health concerns such as mental health, family stress, and even food insecurity.” These pressures are visible in her research site in Mbale, where environmental shocks, economic hardship, and family instability persistently shape daily life. Recurrent landslides and livelihood disruptions place strain on households, and adolescents facing stress or instability may turn to substances as a coping mechanism, she holds.
From evidence to solutions
Completing her PhD has now shifted Aber’s perspective from documenting problems to identifying solutions for social impact. “Completing my PhD shifted my perspective from simply generating evidence to actively providing solutions,” she observed. “Child health challenges such as substance use, nutrition, and climate-related risks are interconnected. As a researcher, I have become more systems-focused, and as an advocate, I feel a stronger responsibility to ensure evidence informs policies that improve children’s wellbeing.”

For Aber, that responsibility extends to the families whose experiences informed the research. Parents, teachers, and health workers often notice behavioural changes first, even when they feel unprepared to respond. Listening without judgment, recognising warning signs, and linking children to appropriate support can make a significant difference, she noted, especially in a context where formal services remain limited.
Her research ultimately sends a clear message for Uganda’s health system. Children affected by substance use are already present in communities and health facilities. Detecting the problem earlier, strengthening screening systems, and equipping frontline health workers with appropriate tools could significantly improve outcomes for vulnerable children.
Behind the research journey stood a wide network of support, including MakSPH supervisors and doctoral committee, the TREAT consortium, the MakSPH PhD forum, the Health Development Centre secretariat, study participants, research assistants, family and friends, and funding support from the Government of Uganda through the Makerere University Research and Innovations Fund (MAKRIF) and the Norwegian Research Council, all of whom she remains grateful.
Aber’s research ultimately points to a critical gap in Uganda’s health system. Children affected by substance use are already present but remain largely invisible. Without routine screening, trained health workers, and clear referral systems, opportunities for early intervention are often missed. Addressing this gap, as indicated by her study, goes beyond clinical care. It requires strengthening how the health system recognises and responds to emerging risks that affect children’s long-term health and development.











The Makerere University College of Health Sciences (MakCHS) on July 10, 2026, welcomed senior six science students from Ngora High School and Wiggins Secondary School to an inspiring Career Fair aimed at guiding them on careers in health sciences and introducing them to the wide range of academic programmes offered by the College.
The event brought together students pursuing Physics, Chemistry, Biology (PCB) and Biology, Chemistry, Mathematics (BCM), providing them with a unique opportunity to interact with the College leadership, tour laboratories and teaching facilities, and learn first-hand about careers in medicine and other health science disciplines.
Welcoming the students, the College Principal, Prof. Bruce Kirenga, described the College of Health Sciences as one of Africa’s oldest and most distinguished medical schools, with a legacy spanning more than a century.
“We started in 1924, making us one of the oldest medical schools on the continent. You have made the right decision to visit Makerere, and we are delighted to welcome you,” he said.
Prof. Kirenga commended the school administrators and teachers for organizing the visit, noting that exposing learners to university environments early helps them make informed career choices. He explained that the College introduced the Open Day concept after receiving numerous requests from schools seeking career guidance visits.

He congratulated the students for choosing science subjects, describing science as the foundation for solving society’s most pressing challenges.
“You have already made one of the most important decisions by choosing to become scientists. Even more importantly, you have chosen life sciences—a field dedicated to preserving and improving life,” he remarked.
The Principal emphasized that careers in life sciences extend far beyond medicine, encouraging students to remain open-minded as they consider their future.
“Everything that has life requires professionals to keep it healthy—from human beings and animals to crops and the environment. The opportunities are immense, including agriculture, veterinary medicine, biomedical sciences, public health and many other emerging fields.”

He also advised students not to limit themselves to only one academic programme during university applications, recalling instances where highly qualified students narrowly missed admission because they selected only one course.
“Remain open to the opportunities available. Medicine is an excellent profession, but there are many other programmes that are equally rewarding and are shaping the future of healthcare and scientific innovation,” he said.
Prof. Kirenga further encouraged the students to embrace lifelong learning, reminding them that scientific knowledge remains valuable regardless of the career path they eventually pursue.
Addressing the students, the Dean of the School of Medicine, Prof. Annette Nakimuli, acknowledged the growing competition for admission into medical programmes and urged learners to work hard while keeping an open mind about the diverse opportunities available within health sciences.

She explained that admission into the Bachelor of Medicine and Bachelor of Surgery (MBChB) programme has become increasingly competitive due to the rising number of high-performing applicants.
“This year we witnessed unprecedented competition for government sponsorship, with many applicants scoring triple A at Advanced Level and outstanding grades at Ordinary Level. That tells you that you must prepare yourselves to excel academically,” she said.
Prof. Nakimuli noted that while many students aspire to become medical doctors, the health sector today offers numerous innovative programmes that are equally important.
“There are many programmes that parents, teachers and students are still not familiar with. Biomedical Engineering, for example, is one of the exciting fields driving the future of healthcare, yet many students overlook it because they focus only on medicine.”

She encouraged students to explore emerging disciplines that combine medicine, engineering, technology and research, noting that the future of healthcare increasingly depends on multidisciplinary professionals.
The Dean also introduced students to the structure of the School of Medicine, explaining that it comprises twelve academic departments and two specialised units covering a broad spectrum of clinical disciplines, including Internal Medicine, Surgery, Obstetrics and Gynaecology, Orthopaedics, Ophthalmology, Ear, Nose and Throat (ENT), Family Medicine, Anaesthesia and Critical Care, among others.
She explained that students are trained by specialists across these disciplines to become competent general practitioners before pursuing further specialization.
Prof. Erisa Mwaka, the Chair of the Department of Human Anatomy, shared with the students about the School of Biomedical Sciences (SBS). He said the school is one of the four schools that make up the Makerere University College of Health Sciences (MakCHS). As the foundation of medical education, the School provides students with a comprehensive understanding of the biological and molecular sciences that underpin modern healthcare, disease prevention, diagnosis and treatment.

The School comprises several departments, including:
- Human Anatomy
- Biochemistry
- Physiology
- Pharmacology and Therapeutics
- Pathology
- Microbiology
- Medical Illustration
The School offers undergraduate programmes such as the Bachelor of Science in Biomedical Sciences, which equips students with strong laboratory, research and analytical skills, and the Bachelor of Science in Biomedical Engineering, an interdisciplinary programme that integrates engineering, medicine and technology to develop innovative healthcare solutions.
At postgraduate level, the School offers a wide range of master’s and doctoral programmes, including Human Anatomy, Physiology, Pharmacology, Bioinformatics, Immunology and Clinical Microbiology, Health Bioethics, Medical Illustration, Pathology and other biomedical specializations that prepare graduates for careers in research, academia, diagnostics, biotechnology and the pharmaceutical industry. The school also offers a wide range of diploma courses.

Throughout the Career Fair, students interacted with faculty members, toured laboratories and learning facilities, and received guidance on university admission, academic programmes and career prospects within the health sciences.
The Career Fair forms part of the College’s broader outreach programme aimed at nurturing the next generation of healthcare professionals by exposing learners to university life and equipping them with the information needed to make informed academic and career decisions.
-

 General2 days ago
General2 days agoUndergraduate Admission Lists 2026/2027
-
 General5 hours ago
General5 hours agoFreshers’ Joining Instructions 2026/2027
-
 General1 day ago
General1 day agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General2 days ago
General2 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General1 week ago
General1 week agoCall for Erasmus+ Mobility Exchanges between Makerere University and University of Perugia