Health
82% Stressed: Uncovering the Hidden Mental Health Burden Among Kampala’s Taxi Drivers

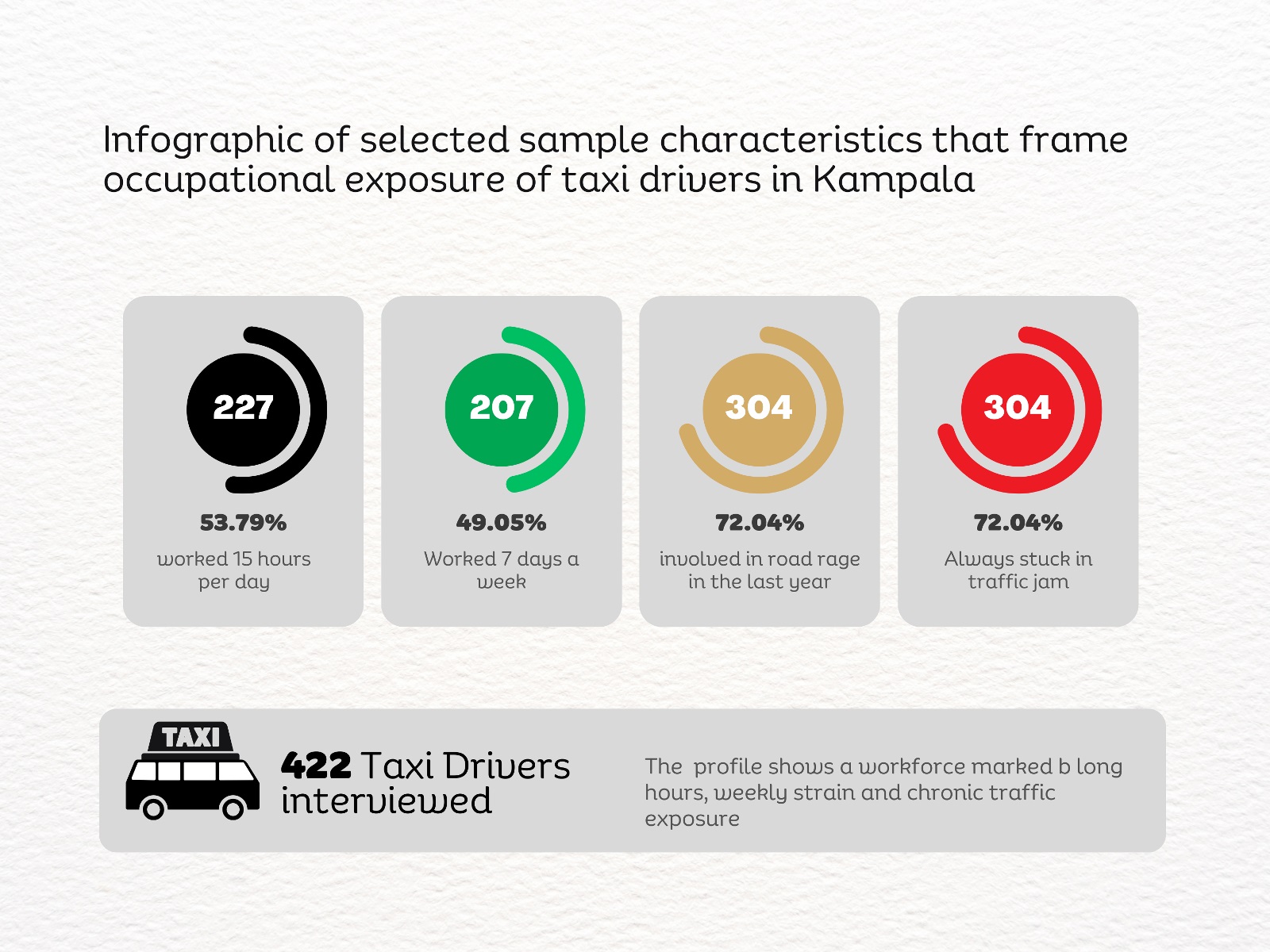
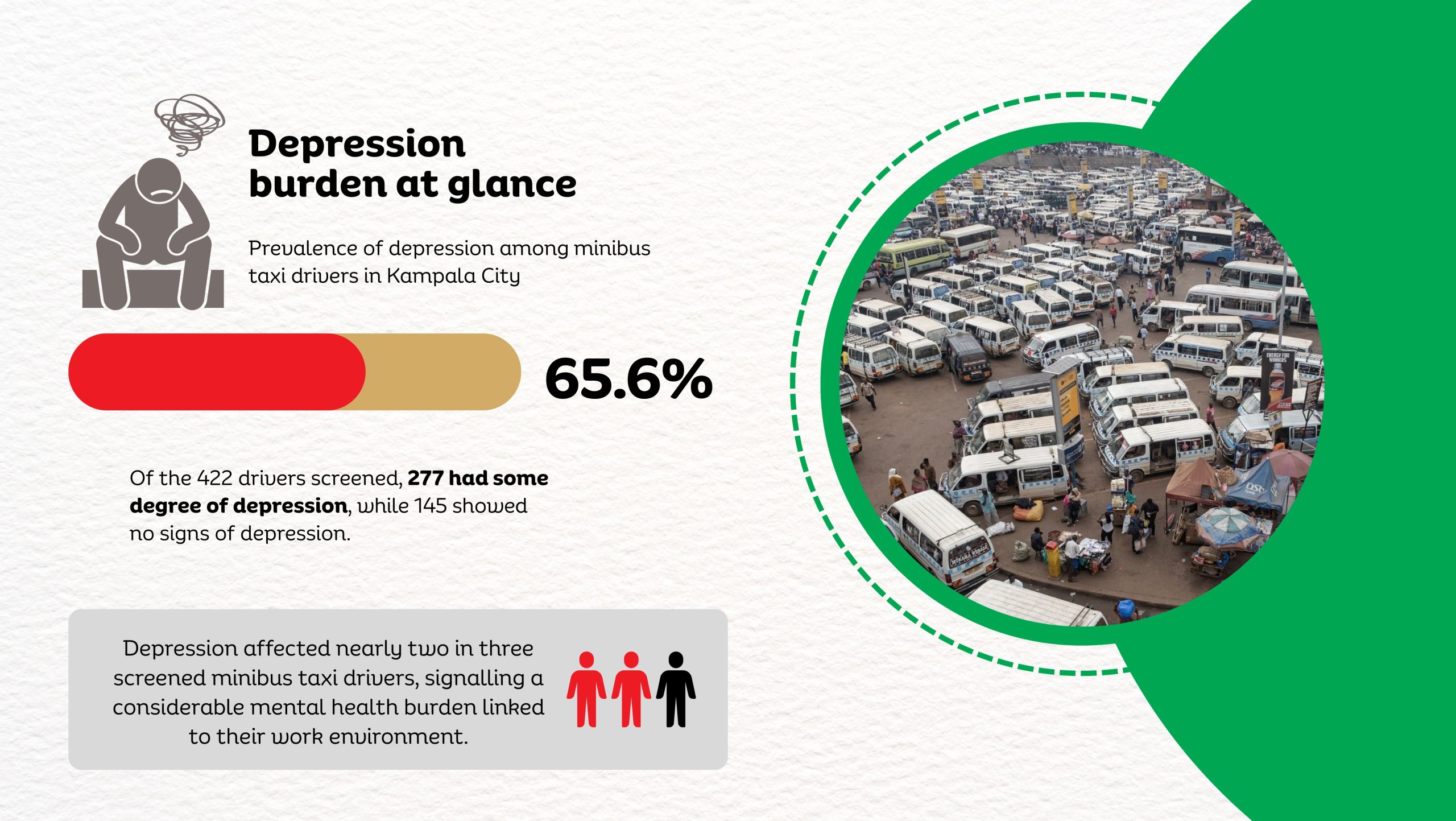
A new study by Dr. Linda Kyomuhendo Jovia, a medical doctor and graduate of the Master of Public Health programme at Makerere University School of Public Health, has found high levels of psychological distress among minibus taxi drivers operating in Kampala’s major taxi parks. In a cross-sectional survey of 422 drivers across Old, New, Kisenyi, Usafi, Namirembe, Nakawa, and Nateete parks, nearly two-thirds screened positive for symptoms of depression (65.6%), while anxiety affected more than 70%, and stress an estimated 82%. The findings point to a largely overlooked occupational health concern within the city’s informal transport sector, where long working hours, economic pressure, poor sleep, and prior road accidents were associated with higher levels of mental strain.
Before sunrise settles over Kampala, Old Taxi Park is already awake. White minibuses marked with the blue stripe of Uganda’s public service taxis sit jammed bumper to bumper, their noses pointed toward narrow exits that will soon release them into the city’s traffic. Dust clings to the windows. Torn seats peek through sliding doors. Diesel hangs low in the air. Conductors slap the metal sides of vans and shout destinations into the morning.
“Kireka! Banda! Bweyogerere!” The calls overlap until they become a steady roar.
Passengers squeeze through narrow corridors between vehicles where there was never meant to be walking space. Hawkers weave through the crowd with trays of roasted maize and boiled eggs. Somewhere, a small radio crackles. Nearby, two conductors argue over whose turn it is to load passengers. This scene is how Kampala wakes, in diesel fumes, shouted destinations, and the quiet urgency of people trying to earn a living before the traffic tightens its grip on the day.
Handwritten route boards fixed to the taxis signal their destinations: Masaka “A” Stage, Kaguta Road, Nakawa, Namirembe, Ntinda, Gayaza, Nansana, and Entebbe, guiding passengers through the organised chaos of the park. Behind every steering wheel sits someone doing the arithmetic of survival. Drivers wake before dawn to secure a place in the queue. For many, sleep is short, interrupted, and rarely restorative. The day stretches across long hours of traffic, uncertain earnings, rent, school fees, and taxi levies, including annual payments of about UGX 720,000. Passengers today mean dinner tonight. Yet inside the noise of the taxi parks, another story has remained largely invisible.
Across Uganda, an estimated 400,000 taxis move millions of passengers every day, forming the backbone of the country’s informal transport system. But almost nothing is known about the psychological toll on the drivers who keep it running.
That gap is what drew Dr. Kyomuhendo into Kampala’s taxi parks. What she uncovered were levels of depression, anxiety, and stress far higher than many had imagined.
A Medical Doctor Turning Toward Public Health
Born on 23 July 1994 to Mr. Muhigwa Lawrence and Ms. Kataito Jacqueline, Dr. Kyomuhendo grew up in Hoima District in western Uganda. Her early education took her from St. Christina Nursery School to Budo Junior School before she continued to Trinity College Nabbingo and later Mount Saint Mary’s College Namagunga for Advanced Level, where she studied Biology, Chemistry, and Mathematics.
In 2014, she earned a government scholarship through the Public Universities Joint Admissions Board and enrolled for a Bachelor of Medicine and Bachelor of Surgery at Busitema University, graduating in 2019.
During her medical internship at Masaka Regional Referral Hospital, she began noticing a troubling pattern in the cases arriving at the wards: road traffic injuries, complications of chronic diseases, severe malaria in children, and obstetric emergencies that might have been prevented with earlier intervention. Many of the crises doctors were treating, she realized, had begun long before patients reached the hospital. “They were symptoms of deeper problems,” she recalls.
Public health offered a way to investigate those underlying causes. In 2022, she enrolled in the Master of Public Health Distance programme at Makerere University School of Public Health, where students are trained to examine health problems not only at the bedside but across entire populations. Guided by Associate Professor Lynn Atuyambe, a respected scholar in Community Health and Behavioural Sciences at MakSPH, and Dr Juliet Kiguli, Senior Lecturer and public health anthropologist, the student’s work benefited from strong academic stewardship.

Uganda’s road transport system is dominated by motorcycles and 14-seater minibus taxis. About 15,000 operate in the Kampala Metropolitan Area alone.
These drivers navigate congested roads, pollution, erratic traffic patterns, and long working hours. Their workday often begins before dawn and stretches deep into the evening.
“They are important in Uganda’s transport industry,” Kyomuhendo said. “Yet they seem to be overlooked in our society.”
While commuting through Kampala during her studies, she began to notice the lives of taxi drivers. Arguments between passengers and conductors were common. When tensions rose, someone would eventually mutter the same question in Luganda.
“Oba abasajja ba takisi baabaki?” loosely to mean, ‘What is wrong with taxi men?’
The question lingered, and in June 2024, social media campaigns marking Men’s Mental Health Awareness Month pushed her to think about the issue differently. What if the behaviour many passengers dismissed as impatience or aggression was linked to something deeper? To her, taxi drivers seemed an unlikely but revealing group to study.
“They carry the responsibility for passengers’ lives every day,” she says. “Yet very little attention is paid to their own well-being.”

For instance, Kampala City Authority (KCCA) documents that between 2019 and 2024, geolocated crash data reveal a dangerous road environment in which Kampala’s taxi drivers operate daily. A total of 1,878 vulnerable road users, including pedestrians, motorcyclists, and cyclists, were killed in crashes involving motor vehicles, with buses and minibuses linked to 281 deaths, most of them pedestrians (147) and motorcycle occupants (131). Fatalities were heavily concentrated along major corridors such as Jinja Road, Kibuye–Natete Road, Bombo Road, and Ggaba Road, while for pedestrians, the most dangerous segments included Gayaza Roundabout (Kalerwe) and Kyebando Police Post along the Northern Bypass and Entebbe Road, where fatality densities reached 27–28 deaths per kilometer. These patterns highlight the high-risk traffic environments in which taxi drivers work, specifically busy arterial roads and bypass intersections where pedestrians, boda bodas, and public transport vehicles compete for space. These conditions contribute to the broader pressures that shape drivers’ safety, well-being, and mental health.
Research in the taxi parks
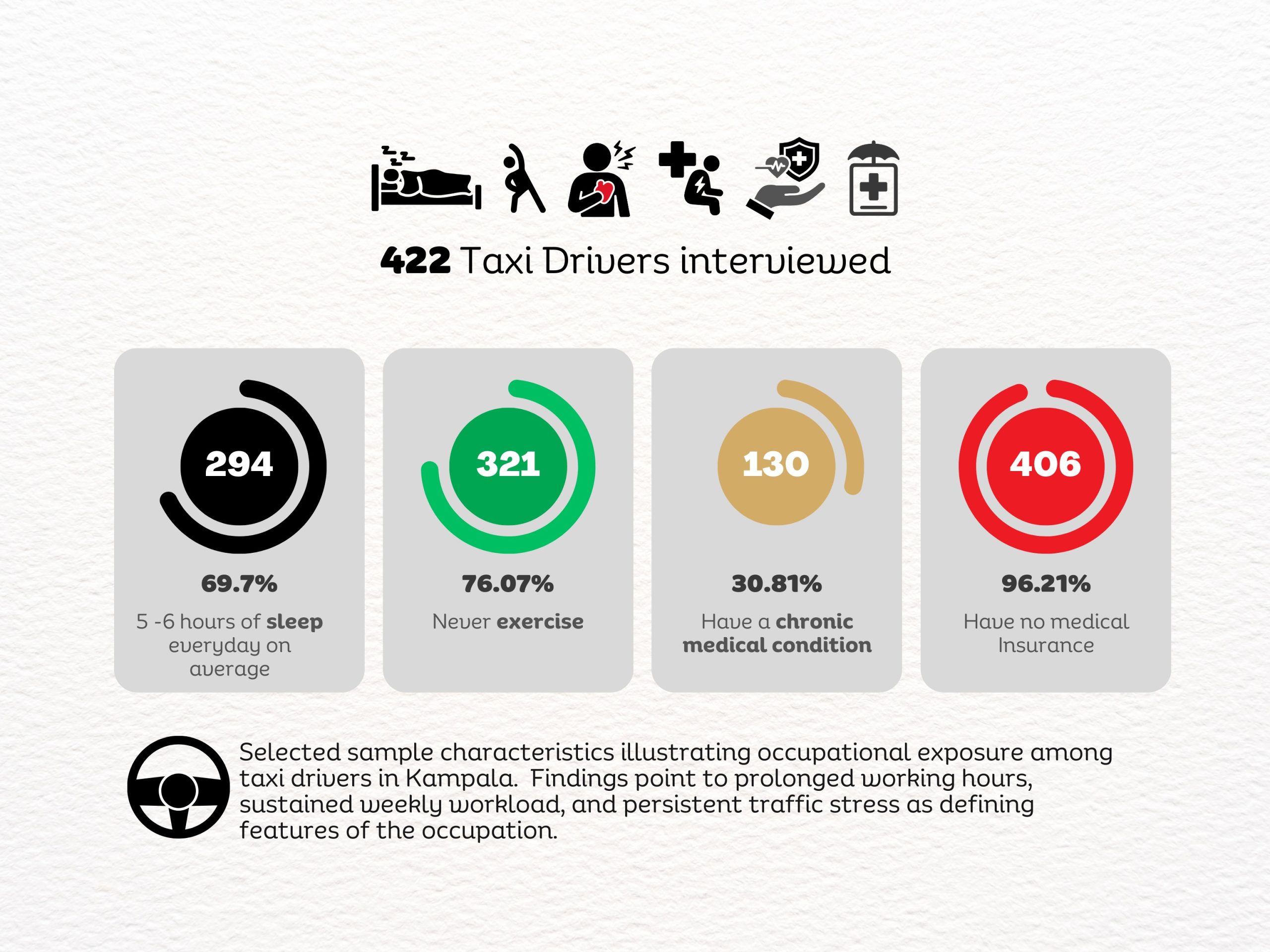
Her dissertation set out to answer two questions: how common are depression, anxiety, and stress among taxi drivers in Kampala, and what factors contribute to them? The study surveyed 422 male drivers across seven major taxi parks: Old, New, Kisenyi, Usafi, Namirembe, Nakawa, and Nateete, using a multistage sampling approach designed to ensure representation across the city’s transport hubs.
Participants completed structured interviews on socio-demographic, occupational, lifestyle, use of habit-forming substances, medical, and environmental factors. Mental well-being was assessed using the Depression Anxiety Stress Scale (DASS-21), a widely used screening tool in mental health research.
The data were analysed using statistical models that allowed Kyomuhendo to examine how occupational conditions, lifestyle factors, and health status interacted to shape mental well-being.
The study reflected the epidemiological training embedded in MakSPH’s Master of Public Health programmes, where students are encouraged to investigate real-world health challenges through evidence-based research.
Conducting interviews inside the taxi parks meant stepping into one of the most unpredictable environments in the city. “The atmosphere was survival for the fittest,” Kyomuhendo recalls.
Stories behind the statistics
The fieldwork brought moments that stayed with her long after the questionnaires were completed. One driver laughed when asked how he coped with stress. “I don’t drink or smoke,” he said, suggesting that multiple relationships were his way of managing the emotional strain of the job.
The answer was not in the questionnaire, and they both laughed. Yet the moment captured something deeper about life in the taxi parks: humour often hides exhaustion.
Another driver told her he had spent years buying herbal medicine for a hernia that never healed. Every month, he spent close to 100,000 shillings, hoping the treatment would eventually work. She advised him to seek hospital care, a conversation that stayed with her.
“Sometimes people spend far more trying to manage a problem than it would cost to treat it properly,” she explains.
When the data were analysed, nearly two-thirds of the drivers screened positive for symptoms of depression. More than 70 percent had symptoms of anxiety, and over 80 percent reported levels of stress. The psychological burden was far heavier than most people had assumed.
Several factors stood out. Drivers who had experienced road accidents in the previous year were significantly more likely to report depression. Chronic medical conditions and a family history of mental illness also increased the risk.
Sleep deprivation emerged as one of the most important predictors. Drivers who consistently slept fewer than seven hours per night were far more likely to report anxiety and stress. Also, economic security mattered. Drivers who owned their vehicles were substantially less likely to experience anxiety compared to those who rented taxis or paid daily remittance fees to vehicle owners. In other words, psychological distress followed the same lines as economic pressure.
More than a transport problem, and the silence around men’s mental health
The implications extend beyond the drivers themselves, she observed. Mental health affects concentration, reaction time, and decision-making. All abilities that are critical for safe driving in a city known for congestion, unpredictable traffic, and frequent road hazards, including flooding, among others.
“If drivers are anxious or sleep-deprived,” Kyomuhendo explains, “there is a risk they may struggle to follow traffic rules or respond quickly to hazards.”
In a transport system that carries millions of passengers daily, the well-being of drivers becomes a matter of public safety. The findings suggest that mental health among taxi drivers should be treated as both an occupational health issue and a transport policy concern.
During interviews, Kyomuhendo noticed another pattern. Few drivers openly described themselves as depressed or anxious. Instead, stress appeared through jokes, casual references to alcohol or relationships, or long pauses followed by silence.
Men’s mental health remains a difficult subject in many communities. “Men’s mental health is a serious public health issue that should not be ignored,” she says.
Breaking the stigma will require awareness campaigns, stronger occupational protections, and greater attention from both health authorities and transport regulators, she proposes.
A different way of seeing the city?
This research also changed how Kyomuhendo sees Kampala. Where passengers notice congestion or impatience, she now sees the pressures shaping the people behind the wheel. “It made me appreciate the men who show up every day and work hard despite their struggles,” she says.
One driver confided in her about the pressures of the job. “People will not help you unless they know the problems you are facing,” he said.
The city and its drivers
By late afternoon, the taxi parks are as crowded as they were in the morning. Conductors still shout destinations into the traffic. Engines idle in long rows of white vans waiting for passengers. Drivers lean against steering wheels, hoping the next arrival will finally fill the vehicle.
The city keeps moving because they do. Most passengers step into these taxis thinking only about where they are going—work, home, school, or the market. Few stop to consider the pressures carried by the people behind the wheel.

Yet Kyomuhendo’s research suggests that beneath the noise of the taxi parks and those car hoots on the streets lies something far quieter and far less visible: a level of stress, anxiety, and depression that touches not only the drivers themselves but also the safety of the passengers they carry and the communities they serve.
Each morning, the vans will still line up bumper-to-bumper. Conductors will still shout destinations into the traffic. Kampala will still climb inside and move.
If nearly half a million taxis keep Uganda moving every day, who is protecting the minds of the people behind the wheel?











Health
MakCHS 2026 Orientation begins: Freshers Urged to Prioritise Responsibility, Integrity and Academic Excellence

New students joining Makerere University College of Health Sciences (MakCHS) have been urged to embrace responsibility, discipline, integrity and hard work as they embark on their journey towards becoming healthcare professionals.
The call was made during the opening session of the college’s orientation programme that began on the 4th August and will conclude on 7th August 2026. During the session, College leaders including the Principal and Deans welcomed students admitted to study various programmes at MakCHS. The speakers outlined expectations for academic and professional conduct.
The session was moderated by Professor Mark Kaddu, Deputy Dean-School of Medicine. Welcoming the freshers, he stressed the importance of hard work highlighting that ‘your academic documents will speak for you and excellence will open doors’.

The college leaders congratulated the students on securing admission to Makerere University, noting that many qualified applicants were unable to secure places. They encouraged the new entrants to make the most of the opportunity by committing themselves to excellence from the first day. The students were reminded that programmes offered by the college are rigorous full-time courses that demand commitment, discipline and consistency.
In his remarks, Professor Bruce Kirenga – Principal, MakCHS welcomed the new entrants and provided an overview of the College’s rich history, highlighting its growth and commitment to excellence in health professionals’ education. The Principal reaffirmed the college’s mission of impacting the national health agenda through transformational teaching, research and innovation for societal development. Students were encouraged to embrace the wide range of career pathways and professional opportunities available upon qualification, emphasizing that their training would equip them to make a meaningful contribution to society.

Stressing the importance of mind-set change which has also been introduced as a crosscutting course, the Principal urged the students to cultivate discipline, resilience, professionalism, and a passion for lifelong learning. “The journey you have embarked on is challenging, but it is achievable,” the Principal noted, reminding the students that many graduates before them successfully completed the programme through dedication and hard work. The address concluded with a call for the new students to remain focused, work diligently, and strive for academic excellence as they prepare to become the next generation of healthcare professionals who will transform their communities.
Professor Annettee Nakimuli, Dean – School of Medicine encouraged students to work collaboratively rather than viewing learning as a competition. She urged them to form productive study groups, support one another and take advantage of opportunities for mentorship, research and international exchange programmes available through the college. “We are here to support you throughout your journey,” she told the students, adding that strong academic performance could open doors to international exchanges, postgraduate training and research collaborations with universities around the world.

Professor Nakimuli warned students against academic dishonesty, including examination malpractice, falsification of academic records and illegal programme changes. She cautioned that such misconduct could lead to dismissal from the university, even after several years of study. Students were further advised to be vigilant against fraudsters who promise to alter admission records or transfer students into different academic programmes through unofficial channels.
In his remarks, Dr. Richard Muhindo, Dean-School of Health Sciences highlighted the importance of personal responsibility and wellbeing beyond academics. He encouraged students to manage their time wisely, avoid drug and alcohol abuse, stay away from gambling and maintain healthy lifestyles throughout their studies. Dr. Muhindo emphasized the importance of professionalism, reminding students that healthcare careers are built on compassion, teamwork and service to humanity. He encouraged students from different programmes to learn together, respect one another’s professions and build networks that will benefit them throughout their careers.

In his address to the freshers, Dr. David Nono who represented Dr. Annet Kutesa, Dean – School of Dentistry, encouraged students to embrace the opportunities before them by working hard, maintaining discipline, and striving for academic excellence. He emphasised the importance of achieving a strong academic record, noting that outstanding performance opens doors to competitive opportunities and future specialisation. The Dean also urged students to pursue postgraduate studies, reminding them that the dental profession requires highly qualified specialists. Reflecting on his own academic journey, he shared how dedication and continuous learning enabled him to study and work internationally before returning to serve the University. He concluded by encouraging students to remain focused, respect University rules, support one another, and make the most of their time at the institution as they prepare for successful professional careers.
Representing the Dean of the School of Biomedical Sciences, Professor Elisa Mwaka welcomed the freshers and congratulated them on earning admission to the College, urging them to embrace responsibility and discipline as they begin university life. Introducing the School of Biomedical Sciences to students, he explained that it handles core foundational courses like Physiology, Biochemistry, Pathology, Medical Microbiology, Immunology, Molecular Biology, among others that support their academic journey. Professor Mwaka reminded students that success at university depends on personal responsibility, regular class attendance, effective time management, and organised study habits, emphasizing that attendance of at least 80 percent of lectures and practical sessions is required to qualify for examinations. He also encouraged students facing academic or personal challenges to seek guidance from their lecturers early rather than waiting until examination time, and urged them to be punctual, prepare adequately for classes.
Mental health featured prominently during the orientation. Leaders acknowledged that health sciences programmes can be stressful encouraging students experiencing emotional or psychological challenges to seek support early rather than suffering in silence. They also called on students to avoid stigmatizing colleagues facing mental health difficulties.
Students were also cautioned to safeguard their personal belongings, particularly phones and laptops, as they settle into campus life. Officials warned that new students are often targeted by thieves during the first weeks of the academic year.
The opening session for the 2026 orientation concluded with a message of encouragement, with MakCHS leaders expressing confidence that the students would develop into competent, ethical and compassionate healthcare professionals capable of contributing to Uganda’s health sector and beyond.
The Orientation Programme continues until Friday, 7th August, and all students were strongly encouraged to attend every session to give themselves the best possible start to their academic journey. Important topics to be covered include IT services, registration procedures, university policies, mental health and well-being, and awareness and prevention of sexual harassment. These sessions are designed to equip students with the knowledge and support they need to thrive both academically and personally.

-

 General7 days ago
General7 days agoUndergraduate Admission Lists 2026/2027
-
 General5 days ago
General5 days agoFreshers’ Joining Instructions 2026/2027
-
 General6 days ago
General6 days agoAdmission Lists for Postgraduate Programmes 2026/27
-

 General7 days ago
General7 days agoMakerere University Welcomes 2026/2027 Freshers
-

 General6 days ago
General6 days agoProf. Ssali makes strong case for Minutes Writing as MakWC Holds Staff Training