Health
TB in Prisons Eight Times Higher Risk than General Population in Uganda, Study

Nearly half of Uganda’s prison population has latent tuberculosis (TB), according to the latest Uganda National Prevalence Survey on Tuberculosis, HIV, and COVID-19. The survey, released on May 15, 2025, found that active TB cases in prisons stand at 1,900 per 100,000—eight times higher than in the general population.
The survey was conducted by Makerere University School of Public Health (MakSPH) in conjunction with the Uganda Prisons Services (UPS) and the Ministry of Health—with funding from the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and technical support from the U.S. Centers for Disease Control and prevention (CDC)—and purposed to have a more profound understanding of TB to help inform public health programs for this high-risk population.
Dr. Simon Kasasa, a Senior Lecturer at MakSPH and Principal Investigator of this study, stressed that “staying for a longer duration, three years and above, posed a greater risk to TB infection in prison.” He also noted TB infection was much higher among male prisoners (48%) compared to female prisoners (38%) and among those of older age, 65 years and above. Meanwhile, the report noted concerns about excessive numbers in prisons as a key risk factor for TB transmission.

UPS consists of 257 prisons spread over 16 administrative regions with an average prisoner population of 56,400 (95% male), accommodation capacity of 16,612 (340%), and 9,904 staff (29% female).
HIV prevalence among prisoners was also alarmingly high at 11%, twice that of the general population. Notably, female persons in prison (PIP) had the highest HIV rates at 21%, compared to 11% for male PIP and just 2% among prison staff. However, the data also showed a significant drop in overall HIV prevalence within prisons, falling from 15% in 2013 to 11% in 2023, with the most dramatic decline among staff, from 12% to 2%.

Dr. George Tumusinze, a Program Manager and Research Associate, pointed out that although 92% of people with HIV in prisons know their status and 99% are receiving antiretroviral therapy (ART), only 70% have successfully reduced the virus in their bodies, highlighting important issues with how well the treatment is working.

Mr. Samuel Akena, the Deputy Commissioner General of Prisons, echoed these concerns by stating that the survey represents a significant milestone for the Prisons, not only in terms of data collection but also in Uganda’s journey towards achieving equity, justice, and the right to health for all. “This survey is historic. It represents one of the most comprehensive efforts to understand the health status of people in prisons in Uganda.” He emphasized the necessity of a collective and bold response, urging that “the time for piecemeal responses is over.”
Dr. Charles Olaro, Director General of Health Services at the Ministry of Health, emphasized the urgency of the situation, stating, “As we gather today to reflect on the findings of this important survey, we must recognize the urgent need for action in our fight against tuberculosis (TB) in Uganda. Despite our efforts, we are still grappling with the burden of this disease, and our progress toward eliminating it by 2030 has not been as swift as we had hoped.” He pointed out that the survey serves as a critical baseline that will shape future responses and guide resource allocation.

HIV prevalence among prison staff members was the lowest, at just 2%, reflecting a significant achievement in workplace health. Dr. Daniel Byamukama, Head of HIV Prevention at the Uganda AIDS Commission, praised prison authorities for their efforts, noting the remarkable progress over the past decade. In the first survey in 2013, only 34% of HIV-positive staff on treatment had achieved viral load suppression. Today, that figure has reached an impressive 100%, underscoring the impact of sustained prevention and care efforts.
While the prison HIV program has shown effectiveness—evidenced by a drop in prevalence from 15% to 11% among the prisoners over the past decade—Mr. Akena stressed the importance of prioritizing gender-responsive strategies in health interventions.
“Diseases do not recognize bars or borders. They thrive in environments where conditions are poor and resources are scarce. Women in prison face disproportionately higher risks, yet often remain invisible in program planning. This is not acceptable. If we are serious about health equity, we must prioritize gender-responsive strategies — within prison health systems and beyond,” Mr. Akena.

CDC Uganda Director Dr. Adetinuke (Mary) Boyd reinforced the significance of the survey in addressing public health risks. “In Uganda, CDC partners are helping to ensure inmates stay healthy during custody. This work facilitates safe reintegration into their communities, mitigates disease transmission to the general population, and reduces public health risks like untreated TB,” she stated. Dr. Boyd highlighted the role of PEPFAR in tackling critical global health threats, asserting that the survey offers helpful data for enhancing health collaboration within this vulnerable population.
The U.S. CDC has been supporting Uganda Prisons Services to provide comprehensive HIV/AIDS, STI, and TB prevention, care, and treatment services for the last 15 years (2010–2025), totaling over $18,046,263 in investment—including $550,000 to this study alone, through the Makerere University School of Public Health. The program supports capacity building, scale-up, and health system strengthening efforts in HIV/TB testing, care, and support for prisoners and prison staff, plus surrounding communities.

With 80% of prison wards overcrowded and 95% lacking adequate natural ventilation, the conditions in which these individuals live exacerbate the spread of infectious diseases, public health specialists have warned. This survey underlines the urgent need for systemic changes within the prison health system, as well as a commitment to uphold the rights and health of all individuals, regardless of their circumstances.
As Uganda grapples with these alarming statistics, the call to action is clear. Stakeholders must come together to implement effective health interventions, improve screening and treatment protocols, and ensure that the rights of incarcerated individuals are respected. The health of the general population is inextricably linked to the health of those within prison walls, and addressing these challenges is not just a moral imperative but a public health necessity.

Professor Rhoda Wanyenze, one of the investigators and Dean of the School of Public Health, asserts that the Survey findings are a wake-up call for stakeholders to prioritize health equity and justice for society’s most vulnerable members.
Prof. Wanyenze advocated for improved TB screening methods and institutionalization of regular mass TB screening using the WHO-recommended advanced diagnostic tools like digital chest X-rays with Computer-Aided Detection (CAD), as well as molecular diagnostics like GeneXpert and TB LAM, noting that traditional symptom-based screening missed nearly half of TB cases. “The use of molecular diagnostics like GeneXpert significantly improved case detection in our study,” she added, emphasizing the importance of timely diagnosis and treatment.

Uganda Prisons Service, in partnership with the Ministry of Health, has so far installed 14 GeneXpert machines in medium- to high-volume prison health facilities.
While some, including Members of Parliament, have raised concerns about the potential infringement on individual rights through mandatory TB testing in prisons, Dr. James Kisambu, the Commissioner for Prison Health Services, noted that it is now apparent, with these findings, for everyone to appreciate that in such confined settings, the risk of transmission is extraordinarily high. TB testing in these settings is not just a medical practice but also a crucial public health precaution that protects both prisoners and the wider community.
“Prisons are high-risk, high-transmission environments where one undetected case can rapidly escalate into an outbreak. In such settings, the right to refuse testing must be weighed against the right of others to be protected from infection. Mandatory TB screening, when done with dignity and linked to prompt treatment, is not a violation of rights — it is an essential public health measure to protect both people in prison and the communities they return to,” said Dr. James Kisambu.

The researchers from MakSPH were; Dr. Simon Kasasa, Associate Professor Esther Buregyeya, Dr. George Tumusinze, Dr. Simon Walusimbi, Dr. Dick Kasozi, Dr. Ronald Senyonga, John Baptist Bwanika, Prossy Nabaterega and Professor Rhoda Wanyenze.
Additionally, the study team from the Uganda Prisons Service comprised of Dr. Leonard Marungu, Charles Butagasa, Dr. James Kisambu and Dr. Johnson Byabashaiza, the Commissioner General of Prisons.
Finally, Dr. Deus Lukoye, Dr. Julius Ssempiira, Charles Kavuma, Rise Nakityo, Samuel Sendagala, Grace Nantege, Lisa Mills, Dr. Lisa Nelson, Kenneth Mwambi from U.S. CDC Uganda/Atlanta and PEPFAR USG agencies, and George William Kasule, Didas Tugumisirize, Dr. Simon Muchuro, Professor Moses Joloba, Dr. Turyahabwe Stavia from the Uganda Ministry of Health National TB and Leprosy Program (NTLP) completed the team.









In Uganda, children arrive at health facilities every day with fever, cough, injuries or routine illnesses. What health workers rarely recognise is that some of these children are already living with alcohol or other substance use disorders, conditions that complicate diagnosis, delay treatment, and quietly undermine children’s health, development, and long-term wellbeing.
This hidden reality was uncovered by Dr. Harriet Aber Odonga during her doctoral research at Makerere University School of Public Health (MakSPH). Her PhD study, titled “Substance Use among Children in Mbale, Uganda: Health System Landscape and Support Structures,” examined how Uganda’s health system detects and responds to substance use among children aged six to 17 years.
The findings revealed a problem far more widespread than many health workers and caregivers assumed. Nearly one in four children attending health facilities showed signs of alcohol or other substance use problems, with alcohol the most common substance. In the study, a child was classified as having a “probable” substance use disorder when responses to a standard screening questionnaire indicated harmful or dependent patterns of use requiring further clinical assessment.

The discovery adds urgency to an already serious public health challenge. Globally, alcohol and other substance use is responsible for one in five deaths and contributes to more than 200 disease and injury conditions, according to WHO. Across Africa, alcohol alone accounts for 6.4 per cent of all deaths and 4.7 per cent of disability-adjusted life years. In Uganda, alcohol use disorder affects roughly 7.1 per cent of the population and contributes to about 7% of all deaths, while research among young people shows that alcohol exposure often begins early in life.
Despite these risks, most policy and research attention has historically focused on adults and older adolescents. Much less is known about children who begin experimenting with alcohol and other substances earlier in their childhood, a gap Aber set out to examine by studying how Uganda’s health system identifies and responds to substance use among children.

A research question begins
Aber’s interest in the subject began unexpectedly. “I remember seeing a notice calling for PhD students to research child alcohol use,” Dr. Aber recounted. “The phrase struck me immediately. I could not believe that children were drinking alcohol. That moment sparked my curiosity, so I began reviewing the literature on the subject in Uganda. During that search, I came across a study documenting alcohol use among children as young as five years old. That finding was deeply unsettling and raised many questions for me.”
With a longstanding interest in child health, Aber saw the research as an opportunity to investigate a problem that had received little systematic attention. What began as disbelief developed into a doctoral investigation examining how Uganda’s health system identifies and responds to substance use among children. She began her doctoral studies in 2021 at MakSPH under the supervision of Dr. Juliet N. Babirye, Prof. Fred Nuwaha, and Prof. Ingunn Marie S. Engebretsen from the University of Bergen, Norway. She defended her thesis on October 25, 2025, before graduating during Makerere University’s 76th graduation ceremony on February 25, 2026.

Investigating the health system response
Aber’s study examined four key questions. It measured how common substance use disorders are among children visiting health facilities. It assessed whether health facilities are equipped to screen and manage these cases. It evaluated whether screening tools are acceptable to children, caregivers, and health workers. It also examined how families seek help when children begin using substances.
To answer these questions, the research used a mixed-methods design combining quantitative surveys and qualitative interviews. Aber collected data from 834 children attending health facilities in Mbale District, assessed 54 health facilities in the district to determine their readiness to screen and manage substance use disorders, and interviewed health workers, caregivers, and children to understand experiences of care and barriers to seeking help. Additional surveys involving 602 children and 355 caregivers examined help-seeking patterns and support structures.
Quantitative data were analysed to estimate prevalence and identify associated risk factors, while qualitative interviews provided insight into how families, communities and health workers respond when children begin using substances.
What the research found

Data collected between 2023 and 2024 across health facilities in Mbale District in Eastern Uganda showed that substance use among children was far more common than many health workers and caregivers assumed. Alcohol use disorder emerged as the most prevalent form of substance use disorder among children in the study. The analysis also showed that children were significantly more likely to use substances if they were exposed to peer or sibling use, lived in lower-income households, or experienced strained relationships with caregivers.
The research also revealed major health system gaps. Only 19 of the 54 health facilities assessed, representing 35 per cent, met the minimum readiness criteria required to screen, diagnose or manage substance use disorders. Many facilities lacked trained staff, standardised screening guidelines, and clear referral pathways for specialised care.
Aber explained that substance use often goes undetected because it is rarely the primary reason children visit health facilities. “Substance use is hidden,” she asserted, reflecting on evidence from her doctoral study. “While health workers are treating other illnesses, some children coming to these facilities are already struggling with alcohol or other substances.”
She added that early substance use can have lasting consequences for children’s development. “Risk was higher among children exposed to peer or sibling substance use, lower household income, lower caregiver education, and strained child-caregiver relationships. The public should be concerned because early substance use affects brain development, mental health, education completion, and long-term well-being.”
Families often navigate the problem alone

Her research also examined how families and communities respond when children begin using substances. She found formal help-seeking to be rare. Many caregivers relied on informal networks, including relatives, teachers, religious leaders, and local authorities. Health services were seldom the first point of support.
Meanwhile, punitive responses such as discipline or punishment were sometimes used by caregivers attempting to stop the behaviour of substance use among children, but these responses rarely addressed the broader social and family pressures influencing the vice.
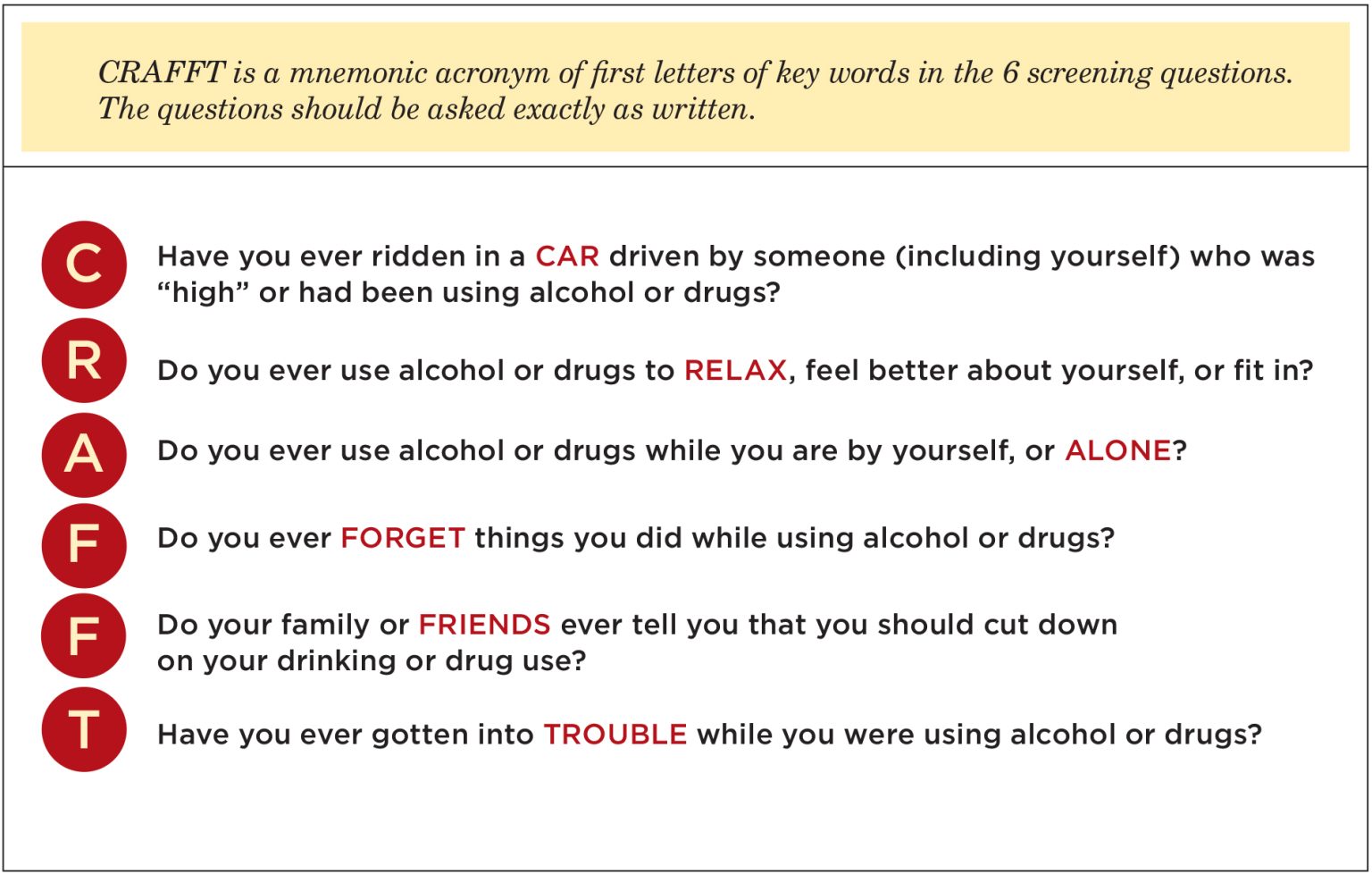
One encouraging finding emerged from her study’s assessment of early detection tools. Aber evaluated the use of the CRAFFT screening tool, a short set of structured questions used by health workers to identify whether a child may be using alcohol or other substances. Children, caregivers, and health workers generally found the questions from the tool easy to understand and acceptable to use. In the study, over 85 per cent of children reported the questions were easy to answer, and nearly nine in ten caregivers were comfortable with the screening process.
These findings, however, suggest that routine early detection could be integrated into primary healthcare within the communities. “If policymakers were to act on one finding from my research, I would prioritise integrating routine, age-appropriate substance use screening into primary healthcare,” Aber argued. “With proper training and referral systems, health workers can identify early risk and support children before the problem escalates.”
Training across nutrition, public health and health systems
Aber’s approach to the problem reflects a research journey shaped by training across multiple areas of child and public health. She first studied Food Science and Technology at Kyambogo University, graduating in 2011, before specialising in Nutrition during her Master of Public Health at Makerere University, graduating in 2015, before embarking on her doctoral training in Public Health at the School, completing in 2025 to graduate at Makerere University 76th Congregation.

Before beginning her PhD, she worked on nutrition research and later coordinated studies examining climate risks, anticipatory humanitarian action and community health systems. This background shaped how she approached substance use among children, not as an isolated behavioural problem but as an issue influenced by broader health and social conditions.
“I do not see child substance use as a problem with a single cause,” she noted. “It is influenced by biological, psychological, social, and system-level factors. My nutrition training helped me appreciate how substance use intersects with broader child health concerns such as mental health, family stress, and even food insecurity.” These pressures are visible in her research site in Mbale, where environmental shocks, economic hardship, and family instability persistently shape daily life. Recurrent landslides and livelihood disruptions place strain on households, and adolescents facing stress or instability may turn to substances as a coping mechanism, she holds.
From evidence to solutions
Completing her PhD has now shifted Aber’s perspective from documenting problems to identifying solutions for social impact. “Completing my PhD shifted my perspective from simply generating evidence to actively providing solutions,” she observed. “Child health challenges such as substance use, nutrition, and climate-related risks are interconnected. As a researcher, I have become more systems-focused, and as an advocate, I feel a stronger responsibility to ensure evidence informs policies that improve children’s wellbeing.”

For Aber, that responsibility extends to the families whose experiences informed the research. Parents, teachers, and health workers often notice behavioural changes first, even when they feel unprepared to respond. Listening without judgment, recognising warning signs, and linking children to appropriate support can make a significant difference, she noted, especially in a context where formal services remain limited.
Her research ultimately sends a clear message for Uganda’s health system. Children affected by substance use are already present in communities and health facilities. Detecting the problem earlier, strengthening screening systems, and equipping frontline health workers with appropriate tools could significantly improve outcomes for vulnerable children.
Behind the research journey stood a wide network of support, including MakSPH supervisors and doctoral committee, the TREAT consortium, the MakSPH PhD forum, the Health Development Centre secretariat, study participants, research assistants, family and friends, and funding support from the Government of Uganda through the Makerere University Research and Innovations Fund (MAKRIF) and the Norwegian Research Council, all of whom she remains grateful.
Aber’s research ultimately points to a critical gap in Uganda’s health system. Children affected by substance use are already present but remain largely invisible. Without routine screening, trained health workers, and clear referral systems, opportunities for early intervention are often missed. Addressing this gap, as indicated by her study, goes beyond clinical care. It requires strengthening how the health system recognises and responds to emerging risks that affect children’s long-term health and development.
By Carol Kasujja and Zaam Ssali
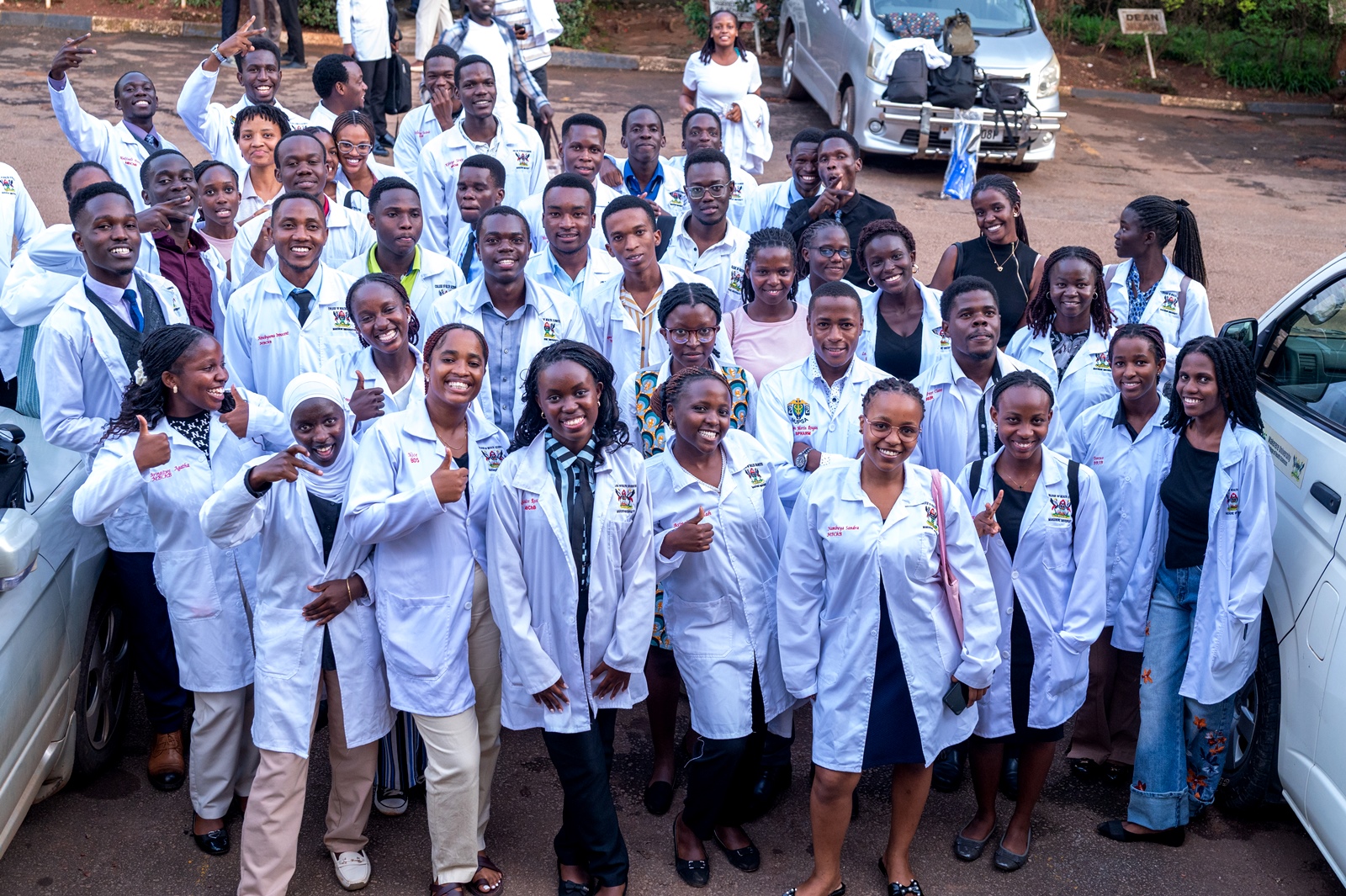
Medical students at Makerere University have been urged to wear the white coat with humility as they begin their journey in the medical profession.
The call was made during the White Coat Ceremony held on Thursday at the Makerere University College of Health Sciences in Mulago.
The White Coat Ceremony marks the beginning of a new journey in healthcare and symbolises professionalism, compassion and excellence. It represents not only the mastery of medical knowledge but also a promise to always place patients at the centre of care. It is a commitment to listen, advocate, heal, and treat every individual with dignity and respect.
“We would have given you a suit, but the symbol of the white coat reminds you that you are here to work. White signifies purity in service. You are in medical school because you are among the best, and you have some of the best lecturers,” said Bruce Kirenga, the Principal of the College of Health Sciences.

Prof Kirenga lauded the students for their dedication to a path dedicated to preserving lives and urged the students to serve with dedication and protect the image of health workers.
“These days, you can use Artificial Intelligence to generate entire coursework, but when it comes to practice, remember the university has an AI policy and you must use it responsibly. In medicine, you take responsibility for your decisions. AI may make life easier, but you must learn and use your hands. Go where the patients are,” he noted.
Prof Kirenga also reminded the students that a medical career offers different paths, including research, teaching, clinical care, and administration.
“As first-year medical students, support each other. Find peers to share your struggles with, especially those in your year. Get mentors and coaches. It took me 26 years to become a Principal, so find mentors who can guide you,” he advised.

Speaking at the event, Sabrina Kitaka, a senior lecturer at the medical school, urged students to uphold the values expected of someone putting on the white coat by being humble and making sure that they connect with their patients.
“Wearing a white coat is a symbol of your commitment to a profession full of honour. This moment is like a rite of passage, from adolescence into adulthood. Joining this noble profession does not make you more important than other students. Be humble,” Dr Kitaka said.
She also encouraged the students to show kindness and compassion to their patients.
Addressing the students, Dr Idro Richard, the Deputy Principal at the College of Health Sciences, called upon the students to always make sure that they keep patients secrets.

“People will come to you and share secrets they have never shared even with their closest family members, do not share people’s pains. If one of you makes a mistake the public will blame all the fraternity so handle your patients with dignity. Always place yourself in the life of those patients when you are in the ward,” Dr Idro, said.
Dr Idro reminded the students to always think of their safety while on the ward by avoiding open shoes.
“Be smart for your own safety, always wear closed shoes, a needle can fall and hurt your legs when you are wearing open shoes. Maintain the excellence you had when you joined and avoid doing life alone,” Dr Idro said.
He further advised the students to always create time and have fun because it is not all about medicine

“Have an open mind, have some fun and also learn other things like soft skills, write, sell and travel. You are in the best School with the best teachers do not allow mediocrity. Avoid cheating, laziness, drugs and betting,” Dr Idro, noted.
In her speech, Anne Atukunda Ronaldine, the chairperson of the Makerere University Medical Students Association (MUMSA), told the first years that they are privileged to join the College as it celebrates a century of excellence.
“Be your brother’s keeper. You will make it together if you work together as a class. Do not avoid your lectures. Medical school is a lot of work, but it gives back,” Atukunda said.

During the ceremony, the College of Health Sciences safeguarding and inclusion champions encouraged students to speak up and report any form of harassment, abuse, or unsafe situations, noting that safeguarding is everyone’s responsibility.
The champions reminded students that creating a safe learning environment requires respect for one another, responsible behavior, and the courage to raise concerns when something is not right. They also urged the new students to support their peers and make use of the available safeguarding channels whenever they feel unsafe or witness misconduct.
The Champions also called upon their peers to support students with disabilities so that no one is left behind. It was a proud moment for many first-year students to finally see themselves wearing white coats, as it was a dream come true for many. The event concluded with a cake-cutting ceremony and a dinner.

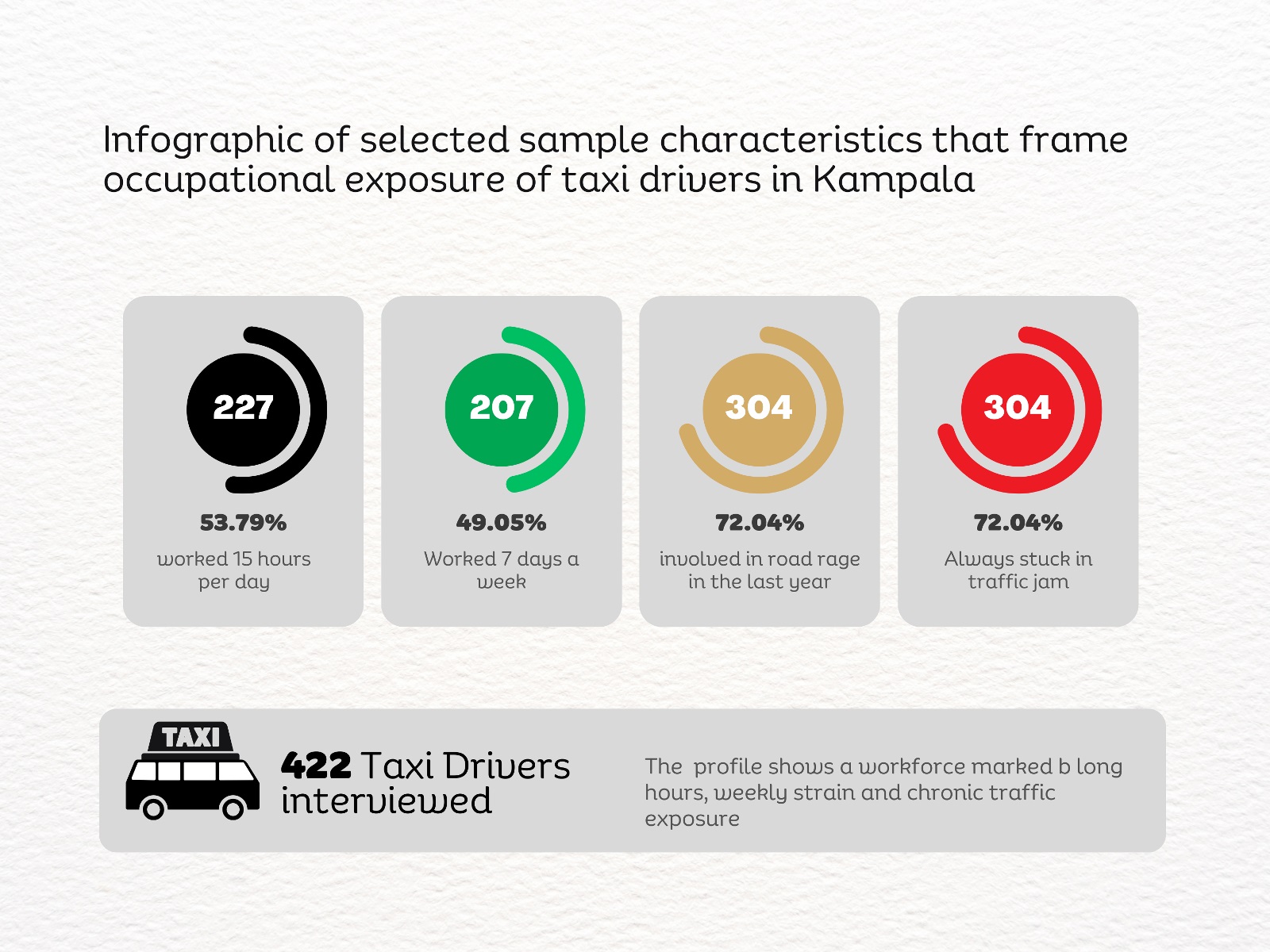
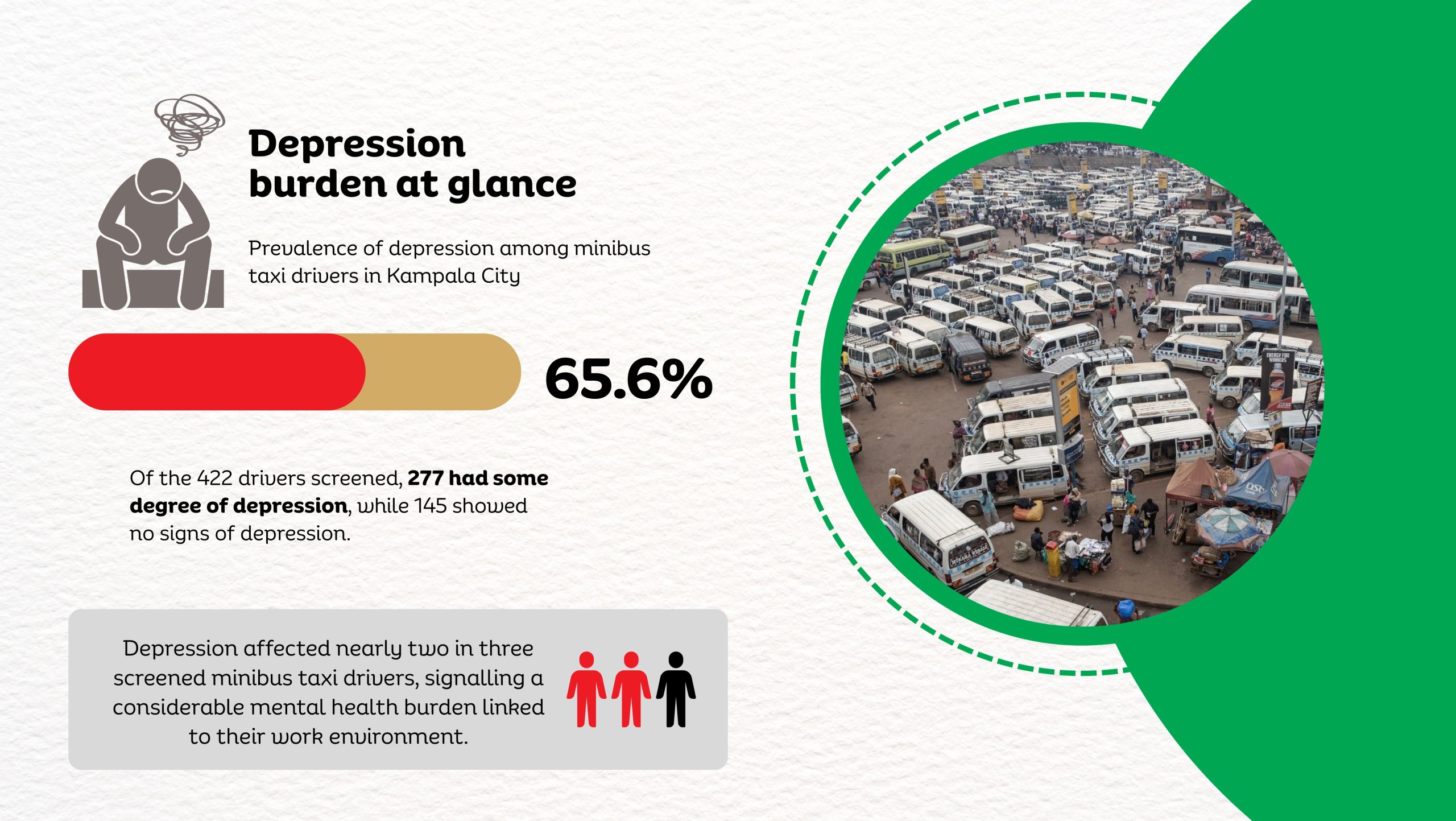
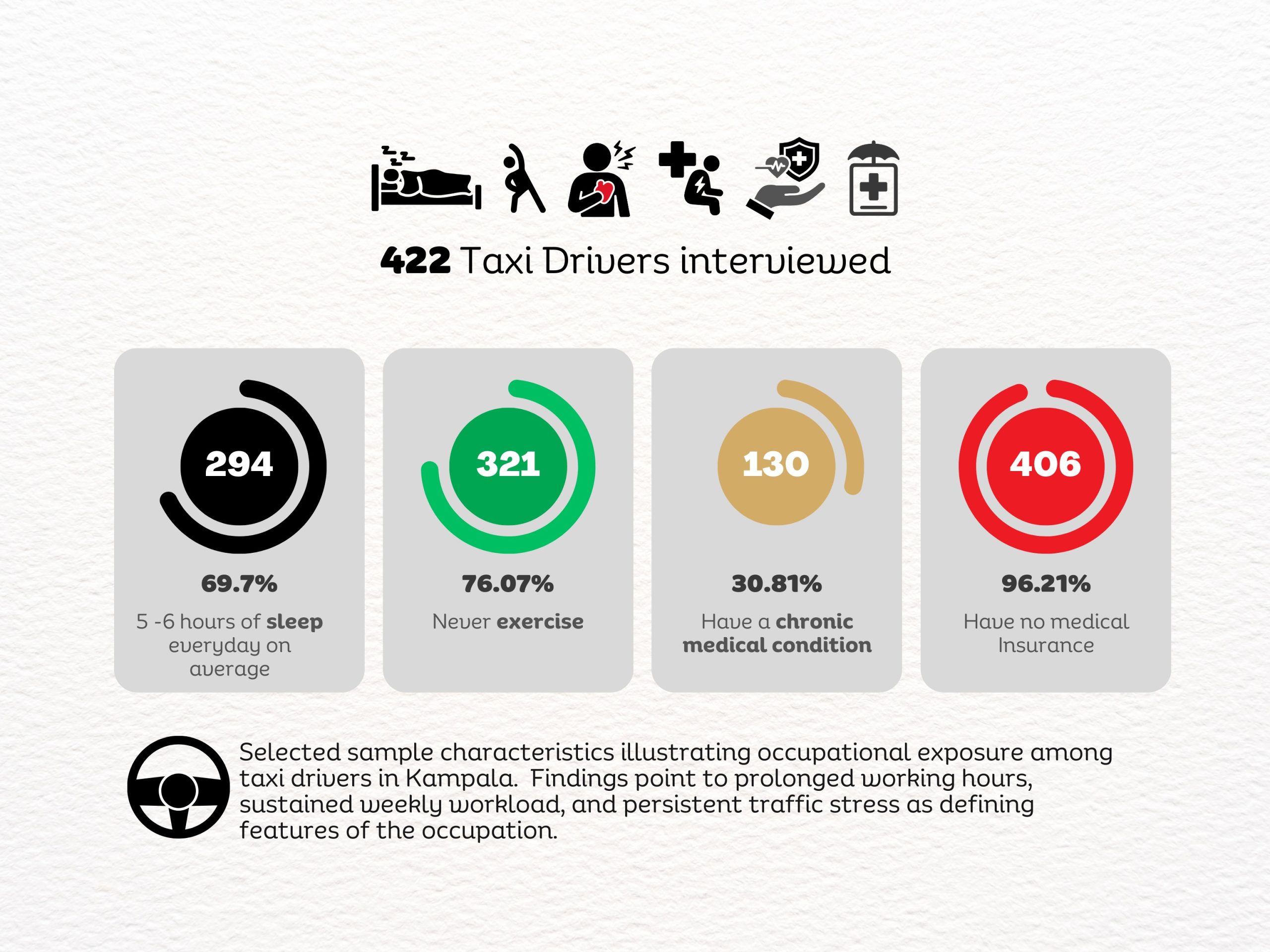
A new study by Dr. Linda Kyomuhendo Jovia, a medical doctor and graduate of the Master of Public Health programme at Makerere University School of Public Health, has found high levels of psychological distress among minibus taxi drivers operating in Kampala’s major taxi parks. In a cross-sectional survey of 422 drivers across Old, New, Kisenyi, Usafi, Namirembe, Nakawa, and Nateete parks, nearly two-thirds screened positive for symptoms of depression (65.6%), while anxiety affected more than 70%, and stress an estimated 82%. The findings point to a largely overlooked occupational health concern within the city’s informal transport sector, where long working hours, economic pressure, poor sleep, and prior road accidents were associated with higher levels of mental strain.
Before sunrise settles over Kampala, Old Taxi Park is already awake. White minibuses marked with the blue stripe of Uganda’s public service taxis sit jammed bumper to bumper, their noses pointed toward narrow exits that will soon release them into the city’s traffic. Dust clings to the windows. Torn seats peek through sliding doors. Diesel hangs low in the air. Conductors slap the metal sides of vans and shout destinations into the morning.
“Kireka! Banda! Bweyogerere!” The calls overlap until they become a steady roar.
Passengers squeeze through narrow corridors between vehicles where there was never meant to be walking space. Hawkers weave through the crowd with trays of roasted maize and boiled eggs. Somewhere, a small radio crackles. Nearby, two conductors argue over whose turn it is to load passengers. This scene is how Kampala wakes, in diesel fumes, shouted destinations, and the quiet urgency of people trying to earn a living before the traffic tightens its grip on the day.
Handwritten route boards fixed to the taxis signal their destinations: Masaka “A” Stage, Kaguta Road, Nakawa, Namirembe, Ntinda, Gayaza, Nansana, and Entebbe, guiding passengers through the organised chaos of the park. Behind every steering wheel sits someone doing the arithmetic of survival. Drivers wake before dawn to secure a place in the queue. For many, sleep is short, interrupted, and rarely restorative. The day stretches across long hours of traffic, uncertain earnings, rent, school fees, and taxi levies, including annual payments of about UGX 720,000. Passengers today mean dinner tonight. Yet inside the noise of the taxi parks, another story has remained largely invisible.
Across Uganda, an estimated 400,000 taxis move millions of passengers every day, forming the backbone of the country’s informal transport system. But almost nothing is known about the psychological toll on the drivers who keep it running.
That gap is what drew Dr. Kyomuhendo into Kampala’s taxi parks. What she uncovered were levels of depression, anxiety, and stress far higher than many had imagined.
A Medical Doctor Turning Toward Public Health
Born on 23 July 1994 to Mr. Muhigwa Lawrence and Ms. Kataito Jacqueline, Dr. Kyomuhendo grew up in Hoima District in western Uganda. Her early education took her from St. Christina Nursery School to Budo Junior School before she continued to Trinity College Nabbingo and later Mount Saint Mary’s College Namagunga for Advanced Level, where she studied Biology, Chemistry, and Mathematics.
In 2014, she earned a government scholarship through the Public Universities Joint Admissions Board and enrolled for a Bachelor of Medicine and Bachelor of Surgery at Busitema University, graduating in 2019.
During her medical internship at Masaka Regional Referral Hospital, she began noticing a troubling pattern in the cases arriving at the wards: road traffic injuries, complications of chronic diseases, severe malaria in children, and obstetric emergencies that might have been prevented with earlier intervention. Many of the crises doctors were treating, she realized, had begun long before patients reached the hospital. “They were symptoms of deeper problems,” she recalls.
Public health offered a way to investigate those underlying causes. In 2022, she enrolled in the Master of Public Health Distance programme at Makerere University School of Public Health, where students are trained to examine health problems not only at the bedside but across entire populations. Guided by Associate Professor Lynn Atuyambe, a respected scholar in Community Health and Behavioural Sciences at MakSPH, and Dr Juliet Kiguli, Senior Lecturer and public health anthropologist, the student’s work benefited from strong academic stewardship.

Uganda’s road transport system is dominated by motorcycles and 14-seater minibus taxis. About 15,000 operate in the Kampala Metropolitan Area alone.
These drivers navigate congested roads, pollution, erratic traffic patterns, and long working hours. Their workday often begins before dawn and stretches deep into the evening.
“They are important in Uganda’s transport industry,” Kyomuhendo said. “Yet they seem to be overlooked in our society.”
While commuting through Kampala during her studies, she began to notice the lives of taxi drivers. Arguments between passengers and conductors were common. When tensions rose, someone would eventually mutter the same question in Luganda.
“Oba abasajja ba takisi baabaki?” loosely to mean, ‘What is wrong with taxi men?’
The question lingered, and in June 2024, social media campaigns marking Men’s Mental Health Awareness Month pushed her to think about the issue differently. What if the behaviour many passengers dismissed as impatience or aggression was linked to something deeper? To her, taxi drivers seemed an unlikely but revealing group to study.
“They carry the responsibility for passengers’ lives every day,” she says. “Yet very little attention is paid to their own well-being.”

For instance, Kampala City Authority (KCCA) documents that between 2019 and 2024, geolocated crash data reveal a dangerous road environment in which Kampala’s taxi drivers operate daily. A total of 1,878 vulnerable road users, including pedestrians, motorcyclists, and cyclists, were killed in crashes involving motor vehicles, with buses and minibuses linked to 281 deaths, most of them pedestrians (147) and motorcycle occupants (131). Fatalities were heavily concentrated along major corridors such as Jinja Road, Kibuye–Natete Road, Bombo Road, and Ggaba Road, while for pedestrians, the most dangerous segments included Gayaza Roundabout (Kalerwe) and Kyebando Police Post along the Northern Bypass and Entebbe Road, where fatality densities reached 27–28 deaths per kilometer. These patterns highlight the high-risk traffic environments in which taxi drivers work, specifically busy arterial roads and bypass intersections where pedestrians, boda bodas, and public transport vehicles compete for space. These conditions contribute to the broader pressures that shape drivers’ safety, well-being, and mental health.
Research in the taxi parks
Her dissertation set out to answer two questions: how common are depression, anxiety, and stress among taxi drivers in Kampala, and what factors contribute to them? The study surveyed 422 male drivers across seven major taxi parks: Old, New, Kisenyi, Usafi, Namirembe, Nakawa, and Nateete, using a multistage sampling approach designed to ensure representation across the city’s transport hubs.
Participants completed structured interviews on socio-demographic, occupational, lifestyle, use of habit-forming substances, medical, and environmental factors. Mental well-being was assessed using the Depression Anxiety Stress Scale (DASS-21), a widely used screening tool in mental health research.
The data were analysed using statistical models that allowed Kyomuhendo to examine how occupational conditions, lifestyle factors, and health status interacted to shape mental well-being.
The study reflected the epidemiological training embedded in MakSPH’s Master of Public Health programmes, where students are encouraged to investigate real-world health challenges through evidence-based research.
Conducting interviews inside the taxi parks meant stepping into one of the most unpredictable environments in the city. “The atmosphere was survival for the fittest,” Kyomuhendo recalls.
Stories behind the statistics
The fieldwork brought moments that stayed with her long after the questionnaires were completed. One driver laughed when asked how he coped with stress. “I don’t drink or smoke,” he said, suggesting that multiple relationships were his way of managing the emotional strain of the job.
The answer was not in the questionnaire, and they both laughed. Yet the moment captured something deeper about life in the taxi parks: humour often hides exhaustion.
Another driver told her he had spent years buying herbal medicine for a hernia that never healed. Every month, he spent close to 100,000 shillings, hoping the treatment would eventually work. She advised him to seek hospital care, a conversation that stayed with her.
“Sometimes people spend far more trying to manage a problem than it would cost to treat it properly,” she explains.
When the data were analysed, nearly two-thirds of the drivers screened positive for symptoms of depression. More than 70 percent had symptoms of anxiety, and over 80 percent reported levels of stress. The psychological burden was far heavier than most people had assumed.
Several factors stood out. Drivers who had experienced road accidents in the previous year were significantly more likely to report depression. Chronic medical conditions and a family history of mental illness also increased the risk.
Sleep deprivation emerged as one of the most important predictors. Drivers who consistently slept fewer than seven hours per night were far more likely to report anxiety and stress. Also, economic security mattered. Drivers who owned their vehicles were substantially less likely to experience anxiety compared to those who rented taxis or paid daily remittance fees to vehicle owners. In other words, psychological distress followed the same lines as economic pressure.
More than a transport problem, and the silence around men’s mental health
The implications extend beyond the drivers themselves, she observed. Mental health affects concentration, reaction time, and decision-making. All abilities that are critical for safe driving in a city known for congestion, unpredictable traffic, and frequent road hazards, including flooding, among others.
“If drivers are anxious or sleep-deprived,” Kyomuhendo explains, “there is a risk they may struggle to follow traffic rules or respond quickly to hazards.”
In a transport system that carries millions of passengers daily, the well-being of drivers becomes a matter of public safety. The findings suggest that mental health among taxi drivers should be treated as both an occupational health issue and a transport policy concern.
During interviews, Kyomuhendo noticed another pattern. Few drivers openly described themselves as depressed or anxious. Instead, stress appeared through jokes, casual references to alcohol or relationships, or long pauses followed by silence.
Men’s mental health remains a difficult subject in many communities. “Men’s mental health is a serious public health issue that should not be ignored,” she says.
Breaking the stigma will require awareness campaigns, stronger occupational protections, and greater attention from both health authorities and transport regulators, she proposes.
A different way of seeing the city?
This research also changed how Kyomuhendo sees Kampala. Where passengers notice congestion or impatience, she now sees the pressures shaping the people behind the wheel. “It made me appreciate the men who show up every day and work hard despite their struggles,” she says.
One driver confided in her about the pressures of the job. “People will not help you unless they know the problems you are facing,” he said.
The city and its drivers
By late afternoon, the taxi parks are as crowded as they were in the morning. Conductors still shout destinations into the traffic. Engines idle in long rows of white vans waiting for passengers. Drivers lean against steering wheels, hoping the next arrival will finally fill the vehicle.
The city keeps moving because they do. Most passengers step into these taxis thinking only about where they are going—work, home, school, or the market. Few stop to consider the pressures carried by the people behind the wheel.

Yet Kyomuhendo’s research suggests that beneath the noise of the taxi parks and those car hoots on the streets lies something far quieter and far less visible: a level of stress, anxiety, and depression that touches not only the drivers themselves but also the safety of the passengers they carry and the communities they serve.
Each morning, the vans will still line up bumper-to-bumper. Conductors will still shout destinations into the traffic. Kampala will still climb inside and move.
If nearly half a million taxis keep Uganda moving every day, who is protecting the minds of the people behind the wheel?
-

 Law7 days ago
Law7 days agoPre-Entry Examination for Admission to the Bachelor of Laws for 2026/2027 AY
-

 General2 weeks ago
General2 weeks agoCall For Applications for Masters Research Support: Drug Safety in Uganda
-

 Research1 week ago
Research1 week agoMakerere Strengthens Research Ethics as Leaders Call for Reforms in Governance, Integrity, and Student Support
-

 General1 week ago
General1 week agoCareer Expo 2026 Concludes as Students Gain Industry Insights, Career Guidance, and Networking Opportunities
-

 General1 week ago
General1 week agoMakerere Hosts Transformative Careers Fair, Bridging Students to the Future of Work