Health
MakSPH Supports Uganda’s Final Push to End HIV with Locally Led Surveillance

In a decisive step toward ending HIV as a public health threat by 2030, Uganda on Thursday, May 29, 2025, officially launched the third Uganda Population-based HIV Impact Assessment (UPHIA 2025) survey, a nationally representative household study expected to provide updated measurements on the status of the HIV epidemic by the end of the year.
The effort is led by Uganda’s Ministry of Health (MoH), with technical assistance from Makerere University School of Public Health (MakSPH), Uganda Bureau of Statistics (UBOS), Uganda Virus Research Institute (UVRI), and the U.S. Centers for Disease Control and Prevention (U.S. CDC), funded by the U.S. government through PEPFAR.
The Population-based HIV Impact Assessment (PHIA) surveys were first launched in 2014 as a global initiative at the International Center for AIDS Care and Treatment Programs (ICAP), based at Columbia University’s Mailman School of Public Health. Supported by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), through the U.S. CDC, the surveys have been conducted in at least 15 high-burden countries globally, including Uganda.
Led by national Ministries of Health, the PHIA surveys provide robust, population-level data on HIV prevalence, incidence, and viral suppression, offering a clear picture of epidemic trends and the effectiveness of national responses. They are designed to track progress, identify persistent gaps, and inform strategies to reach epidemic control, in line with global targets, including the fast-approaching goal of ending AIDS as a public health threat by 2030.

In Uganda, this survey was first rolled out between August 2016 and March 2017. The second followed in February 2020 but was disrupted by the COVID-19 outbreak, continuing through to March 2021. Both rounds were supported by ICAP at Columbia University, which provided technical assistance to strengthen data collection systems, improve laboratory infrastructure, and build national capacity to design, implement, and analyse the two national HIV surveys.
What sets UPHIA 2025 apart is the shift in technical leadership to Ugandan institutions for this third survey, reflecting local capacity to lead rigorous, high-quality public health research. For UPHIA 2025, Makerere University School of Public Health, in partnership with the Uganda Bureau of Statistics and the Uganda Virus Research Institute, is providing technical leadership to the Ministry of Health, alongside U.S. CDC. Implementation began with initial recruitment and training of over 300 field teams that begun on May 19, 2025, ahead of their nationwide deployment for data collection starting this June.
The first survey (UPHIA 2016) was an important milestone in informing Uganda’s national HIV response. This survey, concluded in 2017, measured, among things, the viral load suppression at the population level and provided household-based HIV testing and counselling, with results returned to participants and those who tested positive referred to care. The survey also assessed HIV incidence, HIV and syphilis prevalence, as well as hepatitis B infection rates. These findings would offer nationally representative data to track Uganda’s progress in controlling the HIV epidemic at both national and regional levels.
The next survey, UPHIA 2020, building on past success, was again executed with technical leadership from Columbia University’s ICAP, working with Uganda’s Ministry of Health alongside UVRI, UBOS, regional referral hospitals, local governments, and the U.S. CDC. It offered useful insights that showed encouraging progress, indicating that up to 88% of people living with HIV in Uganda at the time knew their status, 98% of them were on treatment, and 90% had achieved viral suppression. These results reflected momentum toward the UNAIDS global 95-95-95 targets, ensuring that most people living with HIV are diagnosed, treated, and have the virus under control, and advancing the broader goal of ending the epidemic by 2030.
Since the release of these findings nearly five years ago, which helped shape national HIV programming in Uganda, the country has made notable progress, but challenges remain. The UPHIA 2020 findings reported major gaps in testing coverage, particularly among young people and men. The results were also instrumental in identifying service delivery shortfalls and guiding decisions on resource allocation, program design, and policy. Yet today, Uganda remains one of the most heavily burdened countries in the world, with over 1.5 million people living with HIV and over 50,000 preventable new infections recorded per year.

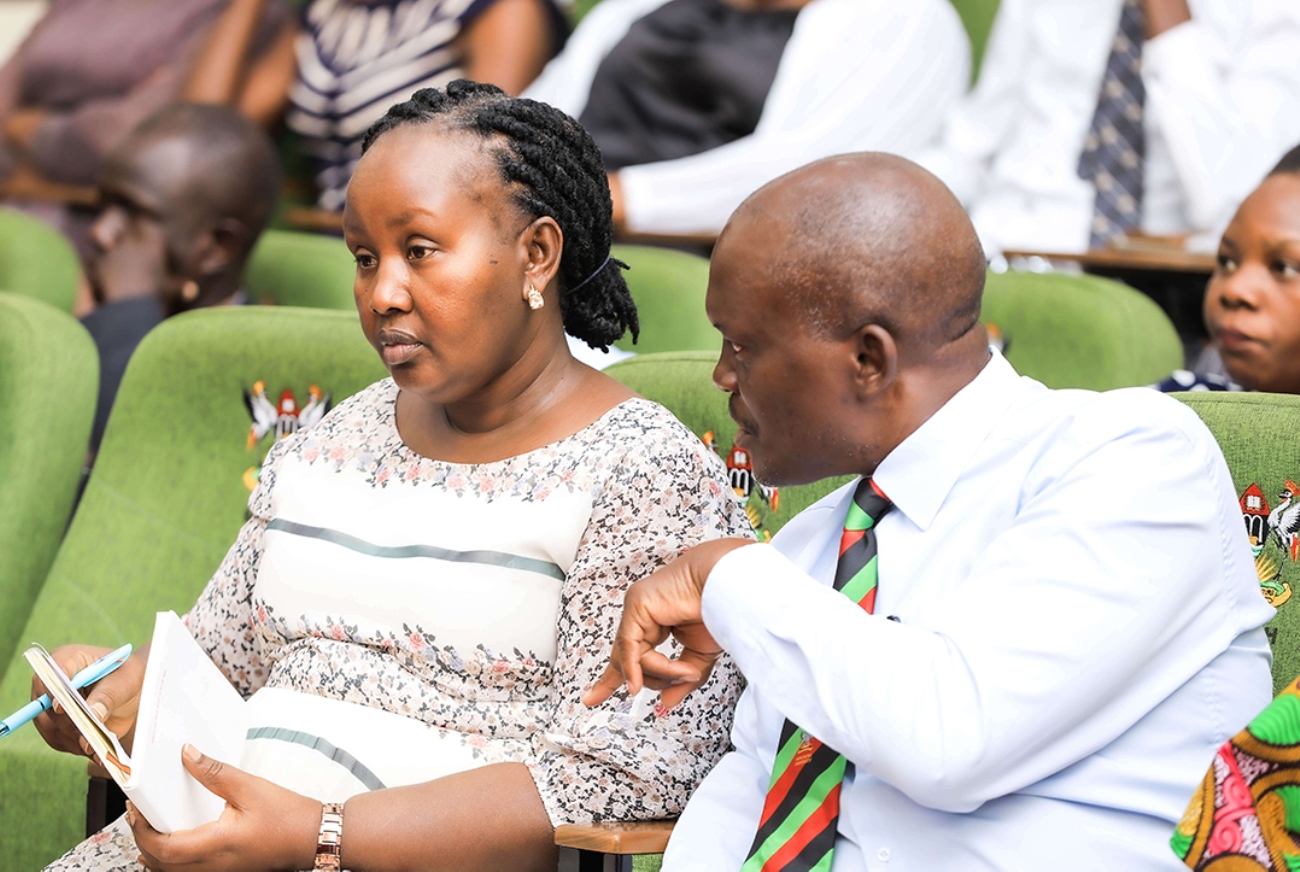
It is this trend that Uganda’s Ministry of Health is working urgently to reverse. Launching UPHIA 2025 at the Ministry’s headquarters in Kampala on May 29, 2025, amidst great hope and expectation among the participants, Uganda’s Minister of Health, Dr. Jane Ruth Aceng Ocero, noted that the long-anticipated and previously delayed survey had arrived at such a critical moment. She welcomed UPHIA 2025 as both a measure of the country’s resilience and a guide for the final stretch toward ending AIDS by 2030, now just a few years away.
“The UPHIA 2025 survey comes at a strategic time to help us recalibrate and refocus our efforts,” the Health Minister said, underscoring the importance of its outcomes. “This will be Uganda’s final population-based HIV survey before 2030, the target year for ending AIDS as a public health threat. The findings will serve as a baseline for tracking our progress toward this national and global goal. They will also guide the next phase of strategic planning, ensuring that the final push toward 2030 is grounded in robust and reliable data.”
This third round of the survey will be carried out in 6,685 randomly selected households across the country. The exercise will involve interviews with approximately 15,000 individuals aged at least 15 and selected through a national household listing by UBOS. Of those, around 14,980 are expected to provide blood samples for HIV testing and analysis of viral suppression and other health indicators. The survey will also include interviews with 1,300 children and adolescents aged 10 to 14, though no blood draws will be taken from this group. Participation is voluntary, free of charge, and requires consent from the head of each household.
Dr. Aceng explained that beyond providing updated estimates of HIV prevalence, incidence, and viral load suppression, and examining regional and demographic disparities, the survey, which will cover the rest of the year, will include a qualitative post-survey assessment component to gather insights from people living with HIV, particularly those not virally suppressed, to understand their challenges and strengthen support services. Also, for the first time, this survey will assess the burden of non-communicable diseases among people living with HIV and include focused interviews with adolescents aged 10 to 14 in Mid-North and Mid-Eastern Uganda, where viral suppression was reported to be lowest in UPHIA 2020.
These activities are made possible thanks to the development support from the U.S. government, which invested $10 million (about UGX 37 billion) for this survey. Speaking at the UPHIA 2025 launch, U.S. Ambassador to Uganda William W. Popp noted that the United States has partnered with Uganda for over three decades to help people live longer, healthier lives;
“The bulk of our annual support, approximately $500 million this year, is dedicated to health programs, making the U.S. government the largest single provider of health assistance to Uganda,” the Ambassador said. He added, “Through PEPFAR, the United States has played a major role in Uganda’s progress toward ending HIV as a public health threat. Since 2003, when Uganda became one of the first countries to implement the program, we have invested nearly three billion dollars—almost 11 trillion Uganda shillings—in HIV prevention, care, and treatment services, saving millions of lives and making both our countries safer from HIV.”

With the benefit of hindsight, Uganda’s early encounter with HIV in the 1980s marked the beginning of one of the region’s most severe epidemics. But over the decades, a determined national response, driven by political leadership, community mobilisation, collaboration and global support, has delivered measurable progress. In the recent past, adult HIV prevalence fell from 7.2% in 2010 to 5.1% in 2023. Among women, it declined from 8.5% to 6.6%, and among men from 5.8% to 3.6%. AIDS-related deaths dropped from 53,000 to 20,000 over the same period, with female mortality declining by 66% and child deaths by 77%.
All these gains, amidst the challenge, go to show what is possible with sustained commitment. What is more, throughout this long journey of Uganda’s battle with eradicating HIV, Makerere University School of Public Health has played a pivotal role. From the early work of Prof. David Serwadda, whose ground-breaking research during the initial detection of HIV helped shape Uganda’s early response, to last year’s 2024 landmark Purpose 1 study on the twice-yearly injectable Lenacapavir that proved 100% efficacy in preventing HIV infection, MakSPH has remained at the forefront of innovation, evidence generation, and policy influence.
That legacy continues today, with the School providing technical leadership to the Ministry of Health in the implementation of UPHIA 2025. At the launch, MakSPH Dean Prof. Rhoda Wanyenze expressed pride in the School’s role as a trusted partner in Uganda’s fight against HIV and other public health challenges. She noted that for over 70 years, during which the School has existed, MakSPH has helped shape the country’s public health landscape through rigorous research, training, and policy support, anchored by a strong, long-standing partnership with the Ministry of Health and partners.

She also noted that the collaboration between Makerere University and the U.S. CDC has helped build national capacity in surveillance and epidemiology, while also strengthening Uganda’s ability to lead high-quality, large-scale national surveys, asserting that:
“The partnership between Makerere University and CDC has not only helped build national capacity in surveillance and epidemiology, but has also strengthened our ability to lead high-quality, large-scale national surveys. After two decades of joint work, we are proud that UPHIA 2024–2025 is now a fully Ugandan-led effort. This is critical to the sustainability of the skills and knowledge generation to inform our local response.”
The survey builds on MakSPH’s experience conducting similar national studies, including those on tuberculosis, prison health, family planning, schistosomiasis, and non-communicable diseases such as the STEPS survey. It will leverage the School’s strong capacity in research and impact evaluation, both in Uganda and across the African region, with a firm commitment to delivering high-quality data guided by the same rigour and integrity that have defined our work over the years, Prof. Wanyenze affirmed.















The Makerere University College of Health Sciences (MakCHS) on July 10, 2026, welcomed senior six science students from Ngora High School and Wiggins Secondary School to an inspiring Career Fair aimed at guiding them on careers in health sciences and introducing them to the wide range of academic programmes offered by the College.
The event brought together students pursuing Physics, Chemistry, Biology (PCB) and Biology, Chemistry, Mathematics (BCM), providing them with a unique opportunity to interact with the College leadership, tour laboratories and teaching facilities, and learn first-hand about careers in medicine and other health science disciplines.
Welcoming the students, the College Principal, Prof. Bruce Kirenga, described the College of Health Sciences as one of Africa’s oldest and most distinguished medical schools, with a legacy spanning more than a century.
“We started in 1924, making us one of the oldest medical schools on the continent. You have made the right decision to visit Makerere, and we are delighted to welcome you,” he said.
Prof. Kirenga commended the school administrators and teachers for organizing the visit, noting that exposing learners to university environments early helps them make informed career choices. He explained that the College introduced the Open Day concept after receiving numerous requests from schools seeking career guidance visits.

He congratulated the students for choosing science subjects, describing science as the foundation for solving society’s most pressing challenges.
“You have already made one of the most important decisions by choosing to become scientists. Even more importantly, you have chosen life sciences—a field dedicated to preserving and improving life,” he remarked.
The Principal emphasized that careers in life sciences extend far beyond medicine, encouraging students to remain open-minded as they consider their future.
“Everything that has life requires professionals to keep it healthy—from human beings and animals to crops and the environment. The opportunities are immense, including agriculture, veterinary medicine, biomedical sciences, public health and many other emerging fields.”

He also advised students not to limit themselves to only one academic programme during university applications, recalling instances where highly qualified students narrowly missed admission because they selected only one course.
“Remain open to the opportunities available. Medicine is an excellent profession, but there are many other programmes that are equally rewarding and are shaping the future of healthcare and scientific innovation,” he said.
Prof. Kirenga further encouraged the students to embrace lifelong learning, reminding them that scientific knowledge remains valuable regardless of the career path they eventually pursue.
Addressing the students, the Dean of the School of Medicine, Prof. Annette Nakimuli, acknowledged the growing competition for admission into medical programmes and urged learners to work hard while keeping an open mind about the diverse opportunities available within health sciences.

She explained that admission into the Bachelor of Medicine and Bachelor of Surgery (MBChB) programme has become increasingly competitive due to the rising number of high-performing applicants.
“This year we witnessed unprecedented competition for government sponsorship, with many applicants scoring triple A at Advanced Level and outstanding grades at Ordinary Level. That tells you that you must prepare yourselves to excel academically,” she said.
Prof. Nakimuli noted that while many students aspire to become medical doctors, the health sector today offers numerous innovative programmes that are equally important.
“There are many programmes that parents, teachers and students are still not familiar with. Biomedical Engineering, for example, is one of the exciting fields driving the future of healthcare, yet many students overlook it because they focus only on medicine.”

She encouraged students to explore emerging disciplines that combine medicine, engineering, technology and research, noting that the future of healthcare increasingly depends on multidisciplinary professionals.
The Dean also introduced students to the structure of the School of Medicine, explaining that it comprises twelve academic departments and two specialised units covering a broad spectrum of clinical disciplines, including Internal Medicine, Surgery, Obstetrics and Gynaecology, Orthopaedics, Ophthalmology, Ear, Nose and Throat (ENT), Family Medicine, Anaesthesia and Critical Care, among others.
She explained that students are trained by specialists across these disciplines to become competent general practitioners before pursuing further specialization.
Prof. Erisa Mwaka, the Chair of the Department of Human Anatomy, shared with the students about the School of Biomedical Sciences (SBS). He said the school is one of the four schools that make up the Makerere University College of Health Sciences (MakCHS). As the foundation of medical education, the School provides students with a comprehensive understanding of the biological and molecular sciences that underpin modern healthcare, disease prevention, diagnosis and treatment.

The School comprises several departments, including:
- Human Anatomy
- Biochemistry
- Physiology
- Pharmacology and Therapeutics
- Pathology
- Microbiology
- Medical Illustration
The School offers undergraduate programmes such as the Bachelor of Science in Biomedical Sciences, which equips students with strong laboratory, research and analytical skills, and the Bachelor of Science in Biomedical Engineering, an interdisciplinary programme that integrates engineering, medicine and technology to develop innovative healthcare solutions.
At postgraduate level, the School offers a wide range of master’s and doctoral programmes, including Human Anatomy, Physiology, Pharmacology, Bioinformatics, Immunology and Clinical Microbiology, Health Bioethics, Medical Illustration, Pathology and other biomedical specializations that prepare graduates for careers in research, academia, diagnostics, biotechnology and the pharmaceutical industry. The school also offers a wide range of diploma courses.

Throughout the Career Fair, students interacted with faculty members, toured laboratories and learning facilities, and received guidance on university admission, academic programmes and career prospects within the health sciences.
The Career Fair forms part of the College’s broader outreach programme aimed at nurturing the next generation of healthcare professionals by exposing learners to university life and equipping them with the information needed to make informed academic and career decisions.
-

 General1 week ago
General1 week agoPress Release: Updates on Makerere University’s Staffing, 2026/7 Academic Calendar, Ebola Response Leadership
-

 General1 week ago
General1 week agoDVCAA Commends RENU Industrial Training Programme, Calls for its Expansion
-

 Agriculture & Environment1 week ago
Agriculture & Environment1 week agoCall for Applications for PhD positions in Dairy Nutrition & Agroforestry
-
 Health2 weeks ago
Health2 weeks agoMakerere University Promotes Prof. Peter Waiswa to Full Professor
-

 Law2 weeks ago
Law2 weeks agoCall for Applications – Makerere University School of Law-Leiden University Exchange Scholarship