Participants pose for a group photo at the "Strengthening leadership and management among local government health managers in Wakiso district, Uganda", Project Dissemination Workshop held on 23rd April 2025 in the MakSPH Auditorium.
Two new studies by researchers at Makerere University School of Public Health (MakSPH) reveal a troubling pattern at the centre of Uganda’s escalating antimicrobial resistance (AMR) crisis, a public health challenge where disease-causing bacteria and other germs stop responding to known medicines meant to kill them, making common infections harder or more expensive to treat.
The studies, conducted in Wakiso and neighbouring districts and recently published in leading scientific journals, examined key drivers of AMR from distinct yet connected perspectives. Together, they expose a health system under strain; shaped by poor-quality medicines circulating in communities, high and often inappropriate antibiotic use in healthcare facilities, and limited public awareness of safe medicine use, conditions now reinforcing one another and accelerating drug resistance.
At the centre, Assoc. Prof. David Musoke, one of the lead researchers on the two studies, and Ms. Bonny Natukunda (Senior Health Educator, Wakiso District) pose with community health workers, district health officials, and facilitators after an AMR workshop in Bukondo, Namayumba Sub-County, on September 22, 2025. Delivered under the NTU–Mak Partnership with Buckinghamshire Healthcare NHS Trust, the week-long workshop trained more than 380 community health workers from Namayumba Sub-County.
According to the Ministry of Health, AMR in Uganda has reached concerning levels. By March 2025, resistant infections were estimated to kill 37,800 people annually, with over 7,000 deaths directly caused by AMR and more than 30,000 linked to infections no longer responding to available treatment. This surge is driven by unrestricted access to antibiotics, weak drug-regulatory enforcement, and widespread misuse of antimicrobials in humans and animals.
The Ministry acknowledges that many patients are treated without diagnostic testing, while low public awareness and weak stewardship across human and veterinary health services continue to fuel microbial resistance. As a result, bacteria that once responded to routine antibiotics now show resistance rates of up to 80 per cent in some cases, undermining treatment outcomes, food safety, and household incomes. It is this challenge that informed the two MakSPH studies.
Part of the study team, led by Assoc. Prof. David Musoke (extreme left), at the recent 10th National AMR Conference in Kampala on November 19, 2025, organised by the Ministry of Health, where they presented evidence from the two studies in Wakiso generated through the NTU–Mak Partnership.
Two Studies, One Warning
Evidence from both studies points to the need for coordinated action to strengthen medicine quality, improve prescribing practices, and build community awareness to preserve the effectiveness of essential treatments. In the first paper, published on October 6, 2025, in the Journal of Pharmaceutical Policy and Practice, researchers led by Associate Professor David Musoke examined how consumers encounter and respond to substandard and falsified medicines for both human and animal use.
Conducted in 2024, the study surveyed 432 community members in Wakiso District, where the Nottingham Trent University – Makerere University(NTU–Mak) Partnership, initiated by NTU’s Prof. Linda Gibson and MakSPH’s Assoc. Prof. Musoke, has implemented community-based health systems programmes for 15 years now. Using a structured household questionnaire, the team assessed knowledge, attitudes, and everyday practices related to medicine use.
NTU’s Prof. Linda Gibson and MakSPH’s Assoc. Prof. David Musoke at the British Academy Equitable Partnerships Workshop on November 20, 2025, reflecting on 15 years of the successful NTU–Mak partnership.
The second study, published on November 21 in the Dovepress Journal of Infection and Drug Resistance, was led by Dr. Bush Herbert Aguma, a pharmacist, health-systems researcher, and Lecturer in the Department of Pharmacy at Makerere University. Working with Assoc. Prof. Musoke and colleagues, the team applied the standardised Global Point Prevalence Survey (GPPS) to examine antibiotic prescribing across three hospitals and five lower-level health centres in Wakiso, Nakaseke, and Butambala. The survey assessed patient demographics, antimicrobial therapy details, and adherence to treatment guidelines to identify gaps requiring improvement.
The surveys were conducted at Entebbe Regional Referral Hospital, Gombe General Hospital, Nakaseke General Hospital, and five lower-level facilities in Wakiso, all part of the Commonwealth Partnerships for Antimicrobial Stewardship (CwPAMS) project at MakSPH implemented through the NTU–Mak Partnership. Alongside the surveys, the partnership has strengthened antimicrobial stewardship in these eight facilities through routine staff training, mentorship, community engagement, and capacity-building in infection prevention and control, microbiology, and detection of substandard and falsified medicines.
“The work was to empower the facility through its Medicines and Therapeutics Committee, which has a sub-committee on antimicrobial stewardship. That committee oversees the process, ensures future surveys are conducted, and can initiate targeted assessments when problems with specific prescriptions arise,” Dr. Herbert Bush Aguma, lead author of the second study, explained.
Dr. Herbert Bush Aguma, explaining the study’s results and impact from his office on December 8, 2025, noted that it has enabled the health facilities to independently track antimicrobial use, identify prescribing gaps, and strengthen stewardship practices.
He added that the programme in the selected facilities for the study went beyond just measuring antimicrobial use, to supporting the facilities develop stewardship plans, strengthening laboratory capacity, and training health workers across human, animal and environmental sectors under a One Health approach. As a result, he stated, facilities can now independently conduct point prevalence surveys, identify prescribing gaps such as inappropriate ceftriaxone use, and advocate for improved diagnostics, while hospitals, Village Health Teams (VHTs), veterinary and environmental officers increasingly address AMR drivers within their settings, leading to significant and lasting impact.
Over the last 15 years, the NTU–Mak Partnership, as part of this work, has trained more than 600 health workers across the human, animal, and environmental sectors in Wakiso, Nakaseke, and Butambala, and equipped over 1,300 community health workers (VHTs) in Wakiso with practical AMR knowledge. University-led programmes, international student competitions, and a 900-member online Community of Practice have further extended its reach. Together, these initiatives demonstrate how sustained community engagement can translate national AMR priorities into real-world impact, offering a model for locally anchored AMR interventions while also supporting the generation of new evidence to strengthen health systems, including the current two studies.
Right: MakSPH student Bridget Ahumuza celebrates a commendation as the 2025 Antibiotic Guardian Health Student of the Year, awarded through the NTU–Mak Partnership for her AMR stewardship advocacy.
What Communities Know, and Don’t Know, About Fake Medicines
In the first study, Assoc. Prof. Musoke and colleagues found that while 83 per cent of respondents had heard of substandard and falsified medicines, only 31 per cent could correctly define the terms, and just seven per cent could accurately identify a falsified product. According to the World Health Organisation (WHO), a global health watchdog, substandard and falsified medicines fail to meet quality standards or deliberately mimic genuine products, often containing the wrong, too little, or no active ingredients. Such medicines put patients at risk of treatment failure, toxicity, and death and accelerate antimicrobial resistance by exposing bacteria to ineffective drug levels.
In Wakiso, the most populous district in Uganda with over 3.3 million people, although over 95 per cent of respondents recognised substandard and falsified medicines as dangerous, many reported having purchased drugs they suspected to be fake: 14 per cent for human and 24 per cent for animal use. To check authenticity, residents relied on advice from health workers or veterinary officers and on buying from trusted outlets. Yet reporting remained extremely low, as only one in four informed a health worker when they suspected a problem, and still, just four per cent had ever reported a case to the National Drug Authority (NDA), mandated to regulate drugs in Uganda.
These patterns reveal a community that recognises the threat of poor-quality medicines but lacks the agency to act. As the study notes, “community members from a range of backgrounds had limited knowledge and poor practices despite commendable attitudes on substandard and falsified medicines… Many respondents reported never having purchased and used substandard and falsified medicines knowingly or unknowingly, although a good number suspected that a medicine they previously purchased had been substandard or falsified.”
Over 50 health managers from 51 healthcare facilities in Wakiso District received certificates at the end of a two-day leadership development training on November 26, 2025, delivered through the NTU–Mak Partnership and Nottingham University Hospitals NHS Trust (NUH) in collaboration with the Wakiso District Local Government and the Ministry of Health. The workshop strengthened leadership capacity across the district health system.
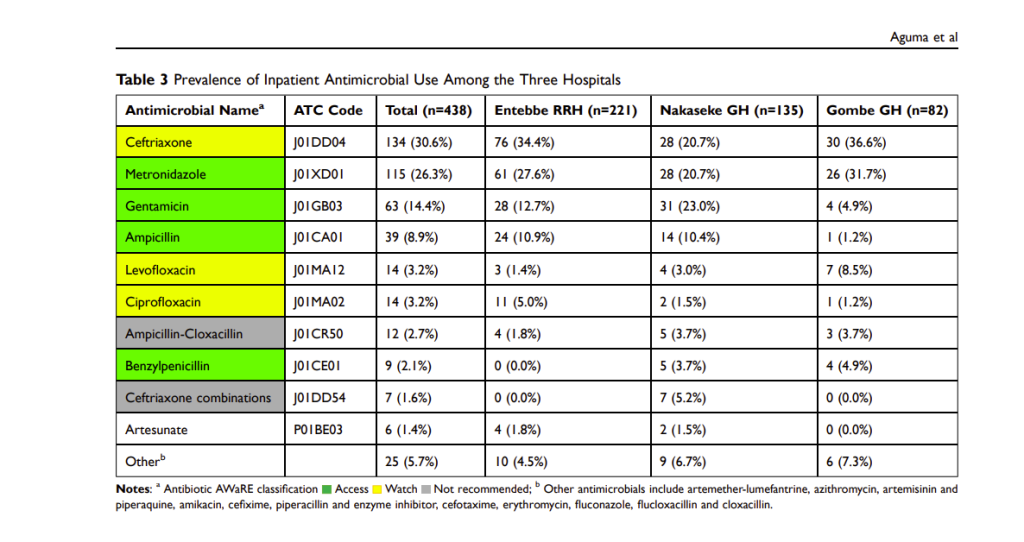
In the second study on antibiotic prescribing, the researchers found high rates of antibiotic use across all eight public facilities. In the three hospitals, 87.2 per cent of inpatients were receiving at least one antibiotic, with ceftriaxone alone, the most commonly prescribed antibiotic in other studies, accounting for nearly one-third of all prescriptions. Most antibiotics were administered prophylactically, especially for obstetric and gynaecological surgeries, which made up 30.7 per cent of all hospital antibiotic use. In lower-level facilities, 60.7 per cent of outpatients received antibiotics, with amoxicillin accounting for 39.1 per cent of all prescriptions. Upper respiratory tract infections, many of them viral, were the leading reason for outpatient antibiotic use.
“Resistance to first-line antimicrobials increases the risk of morbidity and mortality. Unfortunately, the global rise in AMR has not been matched by the development of new antibiotics effective against resistant bacteria,” reads the paper in part. “As a result, healthcare costs are expected to rise, economic productivity will fall due to reduced workforce activity, and global life expectancy could drop by an estimated 1.8 years. This existential threat must be averted to avoid a post-antibiotic era in which even minor infections become fatal.”
In the study on antibiotic prescribing, the researchers found high rates of antibiotic use across all eight public health facilities, with ceftriaxone as the most commonly prescribed antibiotic.
Read together, the two studies provide a ground-level view of how AMR takes root long before a patient reaches a hospital or pharmacy. Poor-quality medicines remain widespread yet poorly understood, while health workers operate under heavy workloads, limited diagnostics, and outdated guidelines that make empirical treatment with antibiotics the default option.
These realities echo the warning delivered by Assoc. Prof. David Musoke, during his keynote address at the 10th National AMR Conference in Kampala on November 19, 2025. Speaking at the event organised by the National One Health Platform, institutionalised in 2016 under the Ministry of Health to coordinate AMR efforts, and held to mark World AMR Awareness Week 2025 under the theme Act Now: Protect Our Present, Secure Our Future, he cautioned that Uganda’s fight against AMR will falter unless communities are placed at the centre of national action.
“One in six bacterial infections globally, and one in five in Africa, are now resistant to available antibiotics,” Dr. Musoke said, citing the latest Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2025. “If Uganda is to make real progress, communities must be treated not as recipients of information but as genuine partners in the fight against AMR.”
Assoc. Prof. David Musoke delivers the keynote address at the 10th National AMR Conference in Kampala on November 19, 2025, warning that Uganda’s fight against AMR will stall unless communities are placed at the centre of national action.
What Must Change: Recommendations from the Researchers
To strengthen antimicrobial stewardship, the study on antibiotic prescribing recommends scaling up diagnostic capacity in public facilities so that treatment decisions are based on laboratory evidence rather than broad empirical prescribing, a medical term that means treatment initiated based on a clinician’s “educated guess” and clinical experience, in the absence of a definitive diagnosis or complete information about the specific cause of a disorder. Expanding functional microbiology services, the study says, would reduce reliance on broad-spectrum antibiotics, which accelerates resistance.
The authors also call for strict enforcement of national treatment guidelines, especially in surgical wards where antibiotics are routinely continued longer than clinically required. For them, reducing unnecessary prophylaxis, particularly in obstetric and gynaecological surgery, would go a long way in limiting misuse without compromising patient safety.
They further urge the Ministry of Health to eliminate non-recommended antibiotic combinations from routine use and ensure consistent stock management to prevent missed doses. This, in addition to strengthening Water, Sanitation, and Hygiene (WASH), and Infection-Prevention and Control (IPC) systems, combined with regular stewardship-focused training for prescribers, is highlighted as essential for improving prescribing standards. Finally, they recommend institutionalising routine point prevalence surveys in Uganda to track trends, guide facility-level action, and reinforce accountability for stewardship.
Makerere University students demonstrate proper hand hygiene while engaging residents in an AMR and hygiene awareness outreach in Kamwokya’s informal settlements on April 11, 2025.
On the other hand, to address the widespread circulation of substandard and falsified medicines, the study team call for a nationwide effort to improve public literacy on how to recognise, verify, and report suspicious medical products. The authors also argue that current reporting pathways are largely invisible, leaving most community members unsure of how or where to lodge complaints. Strengthening the National Drug Authority’s visibility and making its reporting mechanisms simple and accessible, in that case, is identified as a critical first step.
They also highlight the need to engage frontline actors, and this includes Village Health Teams, Community Health Extension Workers, veterinary officers, and local leaders, as primary change agents. These trusted community structures, the authors assert, are well-positioned to translate regulatory messages into actionable information than mass-media campaigns alone.
Given the extensive use of suspected counterfeit veterinary medicines, the authors call for strengthened One Health education and a fully integrated communication approach linking human, animal, and plant health risks. They recommend sustained messaging through radio and other local media, supported by community-driven monitoring systems able to empower consumers to act as partners in protecting the medicine supply chain.
Mr. Mathias Sserwanga (extreme right) of Namulonge HCIII in Wakiso district receiving his certificate from Assoc. Prof. David Musoke (2nd right), following a two-day leadership and management training on November 26, 2025, at Makerere University. The programme by MakSPH and partners has helped enhance the capacity of facility in-charges in Wakiso District to improve health service delivery to the people.
Community-led innovations across Uganda are improving access to healthcare, reducing financial barriers and responding to needs that conventional services do not always reach. The Uganda Case Compendium 2026, published by the Social Innovation in Health Initiative (SIHI) Uganda Hub at Makerere University School of Public Health, documents these solutions, their results and opportunities for scale.
Established in 2017, SIHI Uganda identifies, studies and supports locally developed health innovations. By 2026, the Hub had documented 42 projects through research examining their impact, enabling factors and scalability. It has also convened seven national stakeholder workshops and established a fellowship programme that equips innovators with skills in project management, research, entrepreneurship, communication, fundraising and environmental impact assessment.
The compendium presents evidence of reach and impact. The Ishaka Health Plan has enrolled more than 5,000 people in community-based health insurance, enabling over 4,000 members to access healthcare annually. In Kiryandongo, the Opit Kic Widows Group trained 402 volunteers who have provided health information to more than 6,030 refugee and host-community households. Among people living with HIV who received group support psychotherapy, 98% were depression-free after six months. In Mayuge, two sickle cell clinics have been established, 12,500 children screened and 282 enrolled in continuing care, contributing to a reported 53% increase in enrolment.
Spanning maternal and child health, HIV, mental health, disability, gender-based violence, health financing, diagnostics and palliative care, the compendium provides evidence to inform investment, policy uptake and the responsible scale-up of locally grounded solutions.
Makerere University School of Public Health invites applications for two postdoctoral research fellowships under the ACT-PREP Project, a five-year, Africa-led initiative funded by the Global Health EDCTP3 Joint Undertaking. The project seeks to strengthen sustainable, context-responsive research capacity for epidemic preparedness and response across sub-Saharan Africa.
Responsibilities
Each fellowship is a full-time, 18-month appointment based at MakSPH in Kampala. Applicants must apply for one position only. Eligible candidates should be early-career researchers who are nationals of, or based in, sub-Saharan Africa and hold a PhD in a relevant discipline or have completed a post-Master’s Field Epidemiology Training Programme. Applicants should demonstrate a record of peer-reviewed publication and research dissemination. Experience in policy review, qualitative or mixed-methods research and stakeholder engagement is an advantage. Successful fellows will receive mentorship from senior researchers, collaborate with an international consortium of African and European institutions, and contribute to policy-relevant research on epidemic preparedness. A stipend commensurate with qualifications and experience will be provided. Applications should include a motivation letter of up to two pages, a two-page research concept, a detailed curriculum vitae with a publication list and contacts for at least two referees, and at least one recommendation letter.
Qualifications and Desirable Qualities
Eligible candidates should be early-career researchers who are nationals of, or based in, sub-Saharan Africa and hold a PhD in a relevant discipline or have completed a post-Master’s Field Epidemiology Training Programme.
How to Apply
Submit applications to recruitment@musph.ac.ug by 7 August 2026, quoting “ACT-PREP Postdoc – Position 1 or 2” in the email subject line. Interviews are expected around 14 August 2026 in Kampala.
Qualified women and applicants from under-represented groups are strongly encouraged to apply.
Download the full call for detailed requirements and application guidance.
The Makerere University College of Health Sciences (MakCHS) on July 10, 2026, welcomed senior six science students from Ngora High School and Wiggins Secondary School to an inspiring Career Fair aimed at guiding them on careers in health sciences and introducing them to the wide range of academic programmes offered by the College.
The event brought together students pursuing Physics, Chemistry, Biology (PCB) and Biology, Chemistry, Mathematics (BCM), providing them with a unique opportunity to interact with the College leadership, tour laboratories and teaching facilities, and learn first-hand about careers in medicine and other health science disciplines.
Welcoming the students, the College Principal, Prof. Bruce Kirenga, described the College of Health Sciences as one of Africa’s oldest and most distinguished medical schools, with a legacy spanning more than a century.
“We started in 1924, making us one of the oldest medical schools on the continent. You have made the right decision to visit Makerere, and we are delighted to welcome you,” he said.
Prof. Kirenga commended the school administrators and teachers for organizing the visit, noting that exposing learners to university environments early helps them make informed career choices. He explained that the College introduced the Open Day concept after receiving numerous requests from schools seeking career guidance visits.
Prof. Bruce Kirenga.
He congratulated the students for choosing science subjects, describing science as the foundation for solving society’s most pressing challenges.
“You have already made one of the most important decisions by choosing to become scientists. Even more importantly, you have chosen life sciences—a field dedicated to preserving and improving life,” he remarked.
The Principal emphasized that careers in life sciences extend far beyond medicine, encouraging students to remain open-minded as they consider their future.
“Everything that has life requires professionals to keep it healthy—from human beings and animals to crops and the environment. The opportunities are immense, including agriculture, veterinary medicine, biomedical sciences, public health and many other emerging fields.”
A section of senior six students and their students at the career fair.
He also advised students not to limit themselves to only one academic programme during university applications, recalling instances where highly qualified students narrowly missed admission because they selected only one course.
“Remain open to the opportunities available. Medicine is an excellent profession, but there are many other programmes that are equally rewarding and are shaping the future of healthcare and scientific innovation,” he said.
Prof. Kirenga further encouraged the students to embrace lifelong learning, reminding them that scientific knowledge remains valuable regardless of the career path they eventually pursue.
Addressing the students, the Dean of the School of Medicine, Prof. Annette Nakimuli, acknowledged the growing competition for admission into medical programmes and urged learners to work hard while keeping an open mind about the diverse opportunities available within health sciences.
Prof. Annettee Nakimuli.
She explained that admission into the Bachelor of Medicine and Bachelor of Surgery (MBChB) programme has become increasingly competitive due to the rising number of high-performing applicants.
“This year we witnessed unprecedented competition for government sponsorship, with many applicants scoring triple A at Advanced Level and outstanding grades at Ordinary Level. That tells you that you must prepare yourselves to excel academically,” she said.
Prof. Nakimuli noted that while many students aspire to become medical doctors, the health sector today offers numerous innovative programmes that are equally important.
“There are many programmes that parents, teachers and students are still not familiar with. Biomedical Engineering, for example, is one of the exciting fields driving the future of healthcare, yet many students overlook it because they focus only on medicine.”
Students and Teachers pose for a group photo with CHS staff.
She encouraged students to explore emerging disciplines that combine medicine, engineering, technology and research, noting that the future of healthcare increasingly depends on multidisciplinary professionals.
The Dean also introduced students to the structure of the School of Medicine, explaining that it comprises twelve academic departments and two specialised units covering a broad spectrum of clinical disciplines, including Internal Medicine, Surgery, Obstetrics and Gynaecology, Orthopaedics, Ophthalmology, Ear, Nose and Throat (ENT), Family Medicine, Anaesthesia and Critical Care, among others.
She explained that students are trained by specialists across these disciplines to become competent general practitioners before pursuing further specialization.
Prof. Erisa Mwaka, the Chair of the Department of Human Anatomy, shared with the students about the School of Biomedical Sciences (SBS). He said the school is one of the four schools that make up the Makerere University College of Health Sciences (MakCHS). As the foundation of medical education, the School provides students with a comprehensive understanding of the biological and molecular sciences that underpin modern healthcare, disease prevention, diagnosis and treatment.
Prof. Erisa Mwaka with students in one of the teaching spaces.
The School comprises several departments, including:
Human Anatomy
Biochemistry
Physiology
Pharmacology and Therapeutics
Pathology
Microbiology
Medical Illustration
The School offers undergraduate programmes such as the Bachelor of Science in Biomedical Sciences, which equips students with strong laboratory, research and analytical skills, and the Bachelor of Science in Biomedical Engineering, an interdisciplinary programme that integrates engineering, medicine and technology to develop innovative healthcare solutions.
At postgraduate level, the School offers a wide range of master’s and doctoral programmes, including Human Anatomy, Physiology, Pharmacology, Bioinformatics, Immunology and Clinical Microbiology, Health Bioethics, Medical Illustration, Pathology and other biomedical specializations that prepare graduates for careers in research, academia, diagnostics, biotechnology and the pharmaceutical industry. The school also offers a wide range of diploma courses.
Dr. Isaac Magulu Kimbowa from the Department of Pharmacology and Therapeutics (Right) and colleagues interact with the students.
Throughout the Career Fair, students interacted with faculty members, toured laboratories and learning facilities, and received guidance on university admission, academic programmes and career prospects within the health sciences.
The Career Fair forms part of the College’s broader outreach programme aimed at nurturing the next generation of healthcare professionals by exposing learners to university life and equipping them with the information needed to make informed academic and career decisions.























 General2 days ago
General2 days ago


 General2 days ago
General2 days ago
 General1 week ago
General1 week ago